Download
1 / 9
90 likes | 231 Views
Pulmonary Function. Sleep Abnormalites. Ventilatory Control. Disease. Clinical Manifestation (SDB). Asymptomatic

E N D
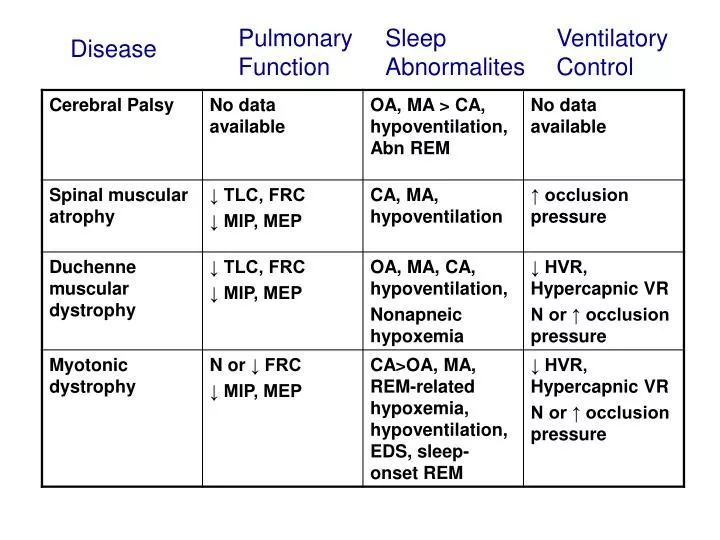
Pulmonary Function Sleep Abnormalites Ventilatory Control Disease
Clinical Manifestation (SDB) • Asymptomatic • Morning headaches, fatigue, exertional dyspnea, irritability, hyperactivity, impaired learning, vomiting, difficulty tolerating supine position, restless sleep [Heckmatt et al 1989, Labanowski et al 1996] • Failure to thrive, nocturnal sweating, developmental delay, cor-pulmonale [Beckerman and Hunt 1992] • These symptoms may be erroneously attributed to the NMD rather than SDB [Gozal 2000] • Nonrestorative sleep and EDS may be the early sign of SDB
Clinical manifestation • PE: Bell shaped chest, tachypnea, use of accessory muscles and paradoxical breathing • Even patients with mild symptoms may have significant unrecognized SDB [Labanowski et al 1996] • Investigations • PFT • Ventilatory control • Polysomnography • Others: Fluoroscopy, CXR, CBC, HCO3
Clinical assessment • PFT • Spirometry, lung volumes, muscle strength assessment • Restrictive physiology • Periodic assessment of PFT especially when lung volumes < 60% [Gozal 2000] • PFT may not be predictive of SDB [Smith et al 1988, Heckmatt et al 1989, Manni et al 1989, White et al 1995] • Other factors contributing to SDB : upper airway, intercostal and diaphragmatic hypotonia, poor airway clearance, pulmonary atelectasis, abdominal distention, GER, pulmonary aspiration, progressive malnutrition or obesity [Givan 2000]
Critical Pulmonary Function Values in NMD Pulmonary Function • FVC < 20 ml/kg ~30% • Vt < 5 ml/kg • FVC < 3 x Vt • MIP < 30 cm H2O • MEP < 40 cm H2O • paCO2> 45 mm Hg Correlation may correlate with elevation of paCO2 awake or asleep
Clinical assessment • Polysomnography • Indication [ATS consensus 1996] : • impaired PFT • snoring, morning headaches, cor-pulmonale, polycythemia and elevated bicarbonate • Planning and implementation of NIPPV • Pre and post-operative evaluation • DMD: annual PSG starting when wheelchair [ATS consensus statement 2004]
Oximetry vs Full PSG • May be useful as a screening test in DMD [Labonowski et al 1996] • In areas where full PSG is not readily available [ATS consensus 2004]
Management • General supportive care : adequate hydration, nutritional support, airway clearance • Scoliosis correction and spinal stabilization • Specific Rx • Elevation of upper body in beds • Rocking bed • Protryptyline: decrease REM-related respiratory disturbances in DMD [Smith et al 1989]