Download
1 / 45
450 likes | 475 Views
Recurrent Oropharyngeal Squamous Cell Carcinoma. Wei Yuan Sodexo Mid-Atlantic Intern 02/04/2013. Objectives. I dentify three risk factors of oropharyngeal cancer . I dentify one major nutrition impact of oropharyngeal cancer. I dentify three major treatments for oropharyngeal cancer.

E N D
Recurrent OropharyngealSquamous Cell Carcinoma Wei Yuan Sodexo Mid-Atlantic Intern 02/04/2013
Objectives • Identify three risk factors of oropharyngeal cancer. • Identify one major nutrition impact of oropharyngeal cancer. • Identify three major treatments for oropharyngeal cancer.
General Information EA 59 YOM African American Admitted to SGAH 01/04/2013 on Med-Surg floor D/C to home 01/10/2013 Readmitted to SGAH 01/15/2013 in ICU Plan to d/c to hospice
Social & Family History Social History Occupation: Not employed Education: High school Marital status: Single w/ a significant other Religion: Baptist Pt currently resides with son in Frederick. History of tobacco, alcohol, cocaine, and other drug abuse. EA just quit smoking a few months ago. Family History His mother died in her 40s because of alcohol abuse. His father died in his 70s due to unknown cause.
Past Medical History Past Medical History Oropharyngeal cancer diagnosed in 2007, status post chemo and radiation therapy. Fungal ball in his left upper lobe of the lung status post antifungal treatment Past Surgery History Gastrostomy tube placement in 2007 The feeding tube was removed 5 months after the placement. Left superficial parotidectomy, left modified radical neck dissection, and wide local excision of recurrent carcinoma on the left side of the face, 08/20/2012. Outpatient medication Fentanyl patch 50 mcg every 72 hrs Ambien 10 mg PO daily
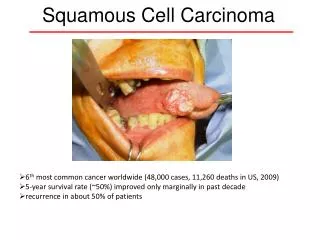
Oropharyngeal Cancer Etiology Oropharyngeal cancer is a disease in which cancer cells are found within the anatomical borders of the oropharynx. The majority of oropharyngeal cancers are squamous cell carcinomas. Major risk factors: tobacco and alcohol abuse. Other risk factors Being infected with human papillomavirus (HPV)-especially HPV-16. Chewing betel quid and drinking mate. Age, gender, poor nutrition, weakened immune system, and genes.
Oropharyngeal Cancer Complications • Airway obstruction • Dysphagia • Disfigurement of the neck or face • Hardening of the skin of the neck • Loss of voice and speaking ability The Major Nutrition Related Problem • DYSPHAGIA
Stages of Oropharyngeal Cancer No actual stage for recurrent cancer in the TNM system.
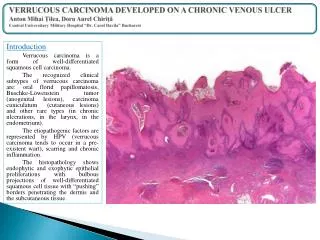
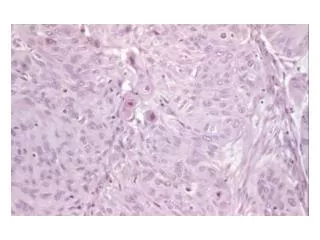
EA's Recurrent Cancer Pathology report, August 2012 Present throughout the parotid gland Moderately differentiated Consistent with recurrent/metastatic carcinoma from primary tumor at the base of the tongue. No carcinoma was identified in eleven lymph nodes.
Admission 1 - Dx & Present Medical Problems Admission Dx Dysphagia secondary to oropharyngeal cancer Oropharyngeal cancer, status post surgery Anemia Hyponatremia Present medical problems Difficulty swallowing x 2 months Finished 7 radiation treatments Significant wt loss (10% in 3 months)
Admission 1 - Procedure Percutaneous Endoscopic Gastrostomy (PEG) on 01/05 Preferred route for head and neck ca patients A lower rate of hospitalization for dehydration A higher therapy completion rate Weight gain or maintenance
Admission 1-Nutrition History Previously having regular diet with good appetite. Soft diet after neck surgery in August, 2012; still good appetite. Swallowing difficulty 2 months ago. Only drinking 3-4 cans Ensure/Boost and 1/2 cup of blenderized soup daily (Estimated energy: 1200 kcal, protein 47 g). Wt loss from 155 lb in Sept. 2012 to 137 lb in Jan. 2013.
Admission 1-Nutrition Assessment Anthropometic Ht: 178 cm Wt: 63 kg BMI: 19.9 IBW: 75.5 kg % IBW: 83.4% UBW: 70 kg % UBW: 90% Wt change: 10% in 3 months Subjective/Objective Soft diet and good appetite until having dysphagia On Osmolite 1.2 at 40 ml/hr when visiting Complaining watery stool x2
Admission 1-Estimated Needs Energy needs range: 30-35 kcal/kg Estimated energy: 1890-2205 kcal Protein needs range: 1.3-1.5 g/kg Estimated protein: 82-95 g Fluid needs range: 1 ml/kcal Estimated fluid needs: 1890-2205 ml
Admission 1-Nutrition Dx (01/09) PES Swallowing difficulty r/t recurrent head and neck ca AEB TF osmolite 1.2 at 40 ml/hrx24 hrs via PEG Involuntary wt loss r/t dysphagia secondary to recurrent head and neck ca AEB 10% wt loss within 3 months. Another possible one Malnutrition r/t dysphagia secondary to recurrent head and neck ca AEB 10% wt loss within 3 months and 1200 kcal po intake before PEG placement.
Admission 1- Goals, Interventions, M/E Nutrition Goals Pt will get adequate nutrition to meet needs from TF with good tolerance Pt will maintain current wt during hospital stay, no further wt loss. Intervention Rec to change TF to Jevity 1.5 at goal rate 60 mlx24 hrs, starting from 35 ml/hr with auto flush water (25ml/hrx24hrs) and extra water 120 ml/every 6 hrs, providing 2160 kcal, 92 g protein, and 2170 ml water. Rec to d/c Miralax and MOM Monitoring & Evaluation TF formula change, rate, tolerance, bowel movement
Admission 1-Follow up (01/10) TF of Jevity 1.5 at 50 ml/hr when visiting Pt reported no N/V, no watery stool, one formed stool since changing formula RN reported no residual A home TF plan needed due to D/C order
Nutrition Goal,Intervention, M/E Goal Pt will understand home TF schedule including formula, rate, and time frame. Intervention Home TF plan: Jevity 1.5, 6 cans per day, one can every 3 hours at 800, 1100, 1400, 1700, 2000, 2300; 178 ml extra water (3/4 cup) to flush the tube every time w/ 1 can of formula (2133 kcal, 91 g protein, and 2149 ml water). If pt tolerates well, TF can be gradually increased to 2 cansx3 times per day. Use an IV pole for gravity TF. Speak w/ case manager regarding TF formula, volume, and the need for an IV pole. Monitoring & Evaluation Understanding of home TF plan
Admission 2 Readmitted on 01/15/2013 Readmitted dx: Acute respiratory failure due to upper airway obstruction Supraglottic edema secondary to radiation therapy Squamous cell carcinoma Anemia Hyponatremia
Admission 2-Procedure Tracheostomy (01/16/2013) EA still wished to continue with radiation therapy for ca An alternative airway After the surgery, EA was sent to ICU, sedated and intubated
Admission 2-Nutrition Assessment (01/18/2013) Anthropometric Ht: 178 cm Wt: 64.4 kg (1.4 kg wt gain since last admission) BMI: 20.3 IBW: 75.5 kg % IBW: 85.3% UBW: 70 kg % UBW: 92% Subjective/Objective Pt was vented, without propofol Abdomen soft, non-tender, non-distended, bowel sounds positive Surgical wounds at the left side of his neck Jevity 1.5 at rate 30 ml/hr (MD order)
Admission 2- Estimated Needs (01/18/2013) Estimated Needs: ~1482 kcal (23 kcal/kg) Penn State equation for critically ill, vented, non-obese patients (Ht: 178cm, Wt: 64.4 kg, age 59 y, ventilation in liter per minute 4L/min, the maximum temperature during the previous 24 hours 36.9 degrees Celsius) RMR=Mifflin (0.96)+ventilation per minute (4)x31+Tmax (36.9)x167-6212=1482 kcal Estimated protein range 1.3-1.5 g/kg Estimated protein needs: 84-97 g Fluid need is per MD order in ICU
Admission 2-Nutrition Diagnosis (01/18/2013) PES statement Inadequate TF intake r/t infusion volume not reached AEB TF intake (1080 kcal/day)< estimated energy needs (1482 kcal/day)
Admission 2-Nutrition Goal, Intervention, M/E Nutrition Goal Pt will have adequate nutrition via TF during hospital stay Intervention Rec to change TF w/ Jevity 1.5, goal rate 35 ml/hr x 24 hrs, Prostat 1 pkt TID via PEG, fluid per MD, providing 1476 kcal (1260 kcal from Jevity 1.5, 216 kcal from Prostat), 99 g protein (54g from Jevity 1.5, 45g from Prostat). Fluid is per MD. Monitoring and Evaluation TF rate change, TF tolerance, wt change
Admission 2-Reassessment (01/21/2013) EA was agitated and fought against ventilation during the weekend. Intubated and sedated w/ propofol at 23.3 ml/hr. Per RN, pt tolerated TF well with 80ml residual in 12 hr shift.
Nutrition Reassessment (01/21/2013) Energy needs: ~1516 kcal (23.5 kcal/kg) Penn State: RMR=Mifflin (0.96)+ventilation per minute (4)x31+Tmax (37.1)x167-6212=1516 kcal. Since propofol was running at 23.3 ml/hr, the calories from propofol (23.3x24x1.1=615 kcal) needed to be subtracted. Calories from TF should be 901 kcal. Estimated protein needs range: 1.3-1.5 g/kg Estimated protein needs: 84-97g Fluid is per MD
Admission 2-Nutrition Diagnosis (01/21/2013) PES Excessive intake from enteral nutrition r/t propofol use at 23.3 ml/hr AEB tube feeding, prostat, and propofol provide 2091 kcal while patient needs 1516 kcal.
Admission 2-Intervention & M/E Intervention Rec to change TF w/ Jevity 1.5, goal rate 20 ml/hr x 18 hrs, Prostat 5 pkt via PEG, fluid per MD, providing 1515 kcal (540 kcal from Jevity 1.5, 360 kcal from Prostat, and 615 kcal from propofol), 98 g protein (23g from Jevity 1.5, 75g from Prostat). Monitoring and Evaluation TF rate change TF tolerance Propofol rate change
The story continues ... 01/25: Pt was extubated, rec to change TF back to Jevity 1.5 at 60 ml/hrx24 hrs, d/c prostat. 01/30: Carotid blowout due to tumor encasing a carotid artery. Plan to d/c to hospice
Nutrition and Wound Care 3 significant wounds Unhealed surgical incisions since radical neck dissection surgery in August, 2012. Wounds deteriorated since radiation therapy
Antioxidants and Radiation Therapy Radiation therapy is used to eradicate cancer and as a palliative measure to relieve pain associated by increasing DNA damage in tumor cells. Antioxidants protect normal cells by reducing the oxidative modification of DNA, while providing same benefits for cancer cells. High-dose antioxidant supplementation: decreasing local tumor control and shortening the survival of ca pts. Only topical wound care was provided for EA.
Nutrition Role Nutrition intervention benefits EA by: Improving kcal and protein intake Maintaining anthropometric measurements Improving the quality of life
References 1. DeVita VT, Lawrence TS, Rosenberg SA. DeVita, Hellman, and Rosenberg’s Cancer Principles & Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011. 2. American Cancer Society. Oral and Oropharyngeal Cancer. 2011. American Cancer Society. Available at: http://www.cancer.org/cancer/oralcavityandoropharyngealcancer/detailedguide/oral-cavity-and-oropharyngeal-cancer-what-is-oral-cavity-cancer. Accessed January 29, 2013. 3. Ang, KK., Harris, J., Wheeler, R., et al. Human Papillomavirus and survival of patients with oropharyngeal cancer. The New England Journal of Medicine. 2010; 363: 24-35. 4. National Cancer Institute. Oropharyngeal Cancer Treatment. 2013. National Cancer Institute at the National Institute of Health. Available at: http://www.cancer.gov/cancertopics/pdq/treatment/oropharyngeal/Patient/page4. Accessed January 29, 2013. 5. Matthews, CM. Cancer cachexia: Pathophysiology and approaches to management. Support Line. 2010; 32(4):5-8. 6. Arends, J., Bodoky, G., Fearon, K. ESPEN guidelines on enteral nutrition: Non-surgical oncology. Clinical Nutrition. 2006; 25: 245-259. 7. Varkey, P., Tang, WR., Tan, TC. Nutrition in head and neck cancer patients. Seminars in Plastic Surgery. 2010; 24 (3): 325-330. 8. Hejl, A., Furze, A. Transforming care for head and neck cancer patients: A multidisciplinary approach. Support Line. 2010; 32(6): 3-9. 9. Nutrition Care Manual. Oncology Comparative Standards. Available at: http://nutritioncaremanual.org. Accessed January 29, 2013.
References 10. Evidence Analysis Library. Critical Illness (CI) Determination of Resting Metabolic Rate (RMR). Available at http://andevidencelibrary.com/template.cfm?key=1309&auth=1. Accessed January 29, 2013. 11. Martindale, RG., McClave, SA., Vanek, VW., et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patients: Society of critical care medicine and American Society for Parenteral and Enteral Nutrition: Executive Summary. Critical Care Medicine. 2009; 37(5): 1757-1761. 12. Daly, JM., Hearne, B., Dunaj, J., et al. Nutritional rehabilitation in patients with advanced head and neck cancer receiving radiation therapy. American Journal of Surgery. 1984; 148(4): 514-520. 13. Hearne, BE., Dunaj, JM., Daly, JM., et al. Enteral nutrition support in head and neck cancer: tube vs. oral feeding during radiation therapy. Journal of American Dietetics Association. 1985; 85(6): 669-74, 677. 14. Chen, Y., Peterson, SJ. Enteral nutrition formula: Which formula is right for your adult patient? Nutrition in Clinical Practice. 2009; 24(3): 344-355. 15. Barrett, JS., Shepherd, SJ., Gilbson, PR. Strategies to manage gastrointestinal symptoms complicating enteral feeding. Journal of Parenteral and Enteral Nutrition. 2009; 33(1): 21-26. 16. Lawenda, BD., Kelly, KM., Ladas, EJ., et al. Should supplemental antioxidant administration be avoided during chemotherapy and radiation therapy? Journal of National Cancer Institute. 2008; 100: 773-783. 17. Borek, C. Antioxidants and radiation therapy. The Journal of Nutrition. 2006; 134: 3207S-3209S.