Download
1 / 30
300 likes | 312 Views
Glaucoma Treatment in Bangalore | Nelivigi Eye provides the evaluation and treatment of glaucoma and other diseases in Bangalore with excellent skills and experienced faculty.<br><br>To know more, visit: https://www.nelivigieyehospital.com/glaucoma-en-in.htm

E N D
World Glaucoma Week March 8 -14, 2020 THE GLAUCOMA BOOK A Comprehensive Guide To Understand More About Glaucoma Dr. Sirish Nelivigi Medical Director-Nelivigi Eye Hospital
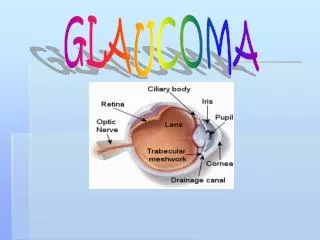
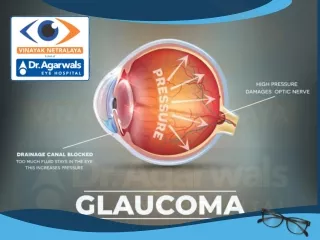
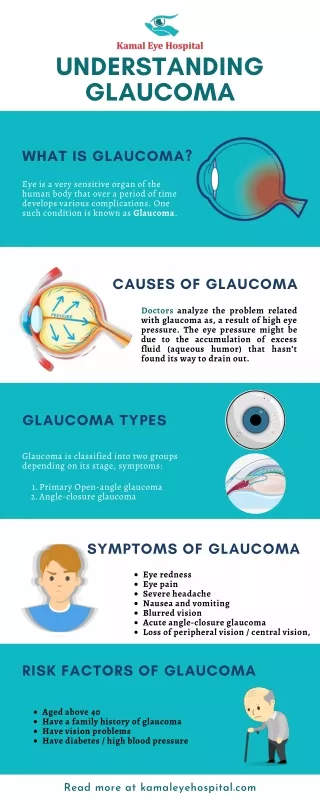
Glaucoma Glaucoma is an optical condition, which is caused by other eye diseases that increase pressure, called the intraocular pressure (IOP) in the eye apparatus in most cases. High pressures are caused by accumulation of excess fluid in the eye, which can cause damage to the optic nerve, if left untreated. Hence early detection, accurate diagnosis and timely treatment are imperative in improving or preserving vision.
Glaucoma The fluid called aqueous humour constantly circulates throughout the anterior chamber of the eye. The aqueous humour is produced by a small gland called the ciliary body, which is located at the rear of the iris. It flows between the lens and the iris and after nourishing the lens and the cornea, seeps out through a sponge-like tissue termed the trabecular meshwork. Its width is just one-fiftieth of an inch and works like the drain of the eye. Nature has placed the trabecular meshwork at the angle where the cornea and iris meet. If the meshwork gets clogged, the aqueous humour cannot drain out of the eye in its normal course and builds up within. Be the ‘sink’ that is the eye is a closed chamber and the ‘water’ cannot overflow. So, the built-up fluid increases pressure in the eye. This is called wide or open angle glaucoma. If excessive air is blown into a balloon, it bursts, but the eye is too strong to burst. The pressure instead, damages the weakest point, a site in the sclera where the optic nerve exits the eye.
Glaucoma The optic nerve carries visual information to the brain. Though it is made up one million nerve cells, it is extremely small in diameter-roughly twenty- thousandth of an inch. When the fluid builds up the pressure, the cells of the optic nerve are compressed. It can result in the death of the nerve cells, which leads to permanent blindness. It cannot be overemphasised that early diagnosis and timely medical intervention can prevent this. The doctor measures the IOP to check for glaucoma.
Types of Glaucoma There are many different forms of glaucoma. The most common types are: � Primary Open-Angle Glaucoma � Normal Tension Glaucoma � Angle-Closure Glaucoma � Acute Glaucoma � Pigmentary Glaucoma � Exfoliation Syndrome � Trauma-Related Glaucoma Let us look at each of these forms of glaucoma
Primary Open-Angle Glaucoma (POAG)
Primary Open-Angle Glaucoma (POAG) POAG occurs mostly in people over fifty. The pressure builds up gradually and the cornea adjusts itself without swelling. Since there are no symptoms to indicate the presence of the condition, it goes undetected. There is no pain and the patient does not realise that his or her vision is slowly deteriorating until the later stages of the condition. However, when vision does get impaired, it is irreversible. There is no perceived abnormality in the trabecular meshwork, but it is believed that due to some reason, its cells may not function normally. There also may be lesser healthy cells due to normal aging. One theory for the condition is a structural defect in the drainage of the aqueous humour. Other experts attribute it to an enzyme dysfunction.
Primary Open-Angle Glaucoma (POAG) All these theories are currently being tested but there is no denying that glaucoma is the result of high IOP. However, not all patients with increased IOP develop glaucoma. Why does high pressures cause glaucoma to develop in some people and not in others is the subject of active research. What we do know is that increased fluid pressure can eventually destroy the cells of the optic nerve. Once enough nerve cells have been decimated, a person sees ‘blind spots’ in the range of vision. They develop initially in the peripheral vision and spread inwards. If left unchecked, it can lead to irreversible blindness. POAG is a chronic disease and may be hereditary; there is no cure for it at present. The only remedy is to slow down vision loss and arrest it eventually. We will see below about the different ways your ophthalmologist can detect glaucoma in the initial stages. However, since there no outward symptoms and the vision is still near-normal, many patients do not understand the necessity of lifelong medication, especially if they have side effects. But taking medications as prescribed is crucial to preserve vision in the long-term.
Normal Tension Glaucoma
Normal Tension Glaucoma Also known as low-tension glaucoma, this disease is a form of POAG. It occurs when there is progressive deterioration of the optic nerve and field of vision but the intraocular pressure is in the normal range. This condition may be related, partially at least to disrupted blood flow to the optic nerve. This kills the cells that carry visual impulses to the brain. Furthermore, the eyes seem to be vulnerable to pressure induced impairment even in high normal IOP range. In such cases the IOP has to be brought down to lower than normal to arrest visual loss. There is a flurry of activity in the field of optic nerve research and its role in progression of glaucoma. There is much optimism about the development of new treatment methods based on the study results. There is no consensus as to the best therapy for normal-tension glaucoma and many of the treatment regimes emerge from the International Collaborative Low-Tension Glaucoma Protocol.
Angle-Closure Glaucoma
Angle-Closure Glaucoma This type of glaucoma is more prevalent among people of Asian descent and those who are farsighted. People vulnerable to developing angle-closure glaucoma have a smaller anterior chamber than average. This constricts the angle where the iris and the cornea meet and where the trabecular meshwork is situated. If the angle is lesser than 45 degrees, the meshwork comes very close to the iris. The lens routinely grows larger as we age. The flow of the aqueous humour between the iris and the lens en route to the anterior chamber is disrupted. This causes fluid build-up behind the iris, which further narrows the angle. If the IOP becomes higher, the iris is pushed against the trabecular meshwork. This is similar to putting a stopper over the drain of a sink. When this space is blocked completely, it causes an angle-closure glaucoma attack (acute glaucoma). Unlike in POAG where the IOP increases gradually, there is a drastic upsurge fluid pressure; it can happen within a few hours.
Painful as it is, the pressure can go up to levels that cause nausea and vomiting. The eye reddens and the cornea swells up and clouds over. The patient experiences blurred vision and sees haloes around light sources. An acute attack of glaucoma is a medical emergency and warrants immediate intervention. If treatment is delayed, there can be permanent loss of vision. If the attack scars the trabecular meshwork, the result could be chronic glaucoma. This condition is much more difficult to stabilise and may lead to the development of cataract. Damage to the optic nerve is quick and could be irreversible. This disease may also be hereditary with several family members being afflicted. Causes of Angle-Closure Glaucoma Many sudden angle-closure glaucoma ‘attacks’ occur in darkened rooms like movie theatres. As we have seen, darkness causes the pupil to dilate or expand, which brings the lens of eye and the iris in closest contact. This narrows the angle even further, which may trigger an attack. However, the pupil also dilates in times of excitement or anxiety. Hence, the onset of this disease can also coincide with periods of stress or extreme nervousness
Causes of Angle-Closure Glaucoma Furthermore, there are many drugs, which also cause the pupil to expand. These include cold medications, anti-depressants, antihistamines and certain medications for nausea. Most of the attacks do not cause major disruptions; sometimes, the patient may have a succession of minor attacks. The attacks may manifest as slightly blurred vision and seeing haloes; haloes are seen as rainbow-coloured rings surrounding lights. There may no pain or redness. The attacks can end once the patient enters a well-lit room, which immediately constricts the pupil. Constriction causes the iris to pull away from the lens. Some people may become afflicted with chronic angle- closure glaucoma. This is a disease, in which the iris gradually closes over the lens. There are no visible symptoms but scars form slowly between the lens and the iris. The IOP does not rise till a sufficient amount of scar tissue blocks the drainage area. Medication like pilocarpine may prevent an acute attack, but the chronic form of angle-closure glaucoma can still develop.
Causes of Angle-Closure Glaucoma A person’s chances of developing closed-angle glaucoma can be predicted with routine check-ups with a procedure known as gonioscopy. The examination uses a special lens with a mirror, which is lightly placed on the front of the eye and the width of the angle is visually measured. People who have narrow angles can be warned to look out got early symptoms so that can seek immediate medical intervention. Laser treatment may also be recommended as a preventive measure in some cases. If the attack is acute, a combination of drugs helps to constrict the pupil and provide immediate relief. There are some drugs that reduce the production of aqueous humour, thus regulating IOP levels. After this is done, your ophthalmologist may perform a laser iridotomy. It is an outpatient procedure, in which a laser beam makes a tiny opening in the iris. This opening enables the humour to circulate freely. It is also a painless procedure, before which local anaesthesia is given with drops and the entire procedure takes less than a half-hour. However, it is common for narrow-angle glaucoma to afflict both eyes. Hence as a preventive measure, the ophthalmologist may operate on the healthy eye as well.
Pigmentary Glaucoma Pigmentary glaucoma is a hereditary form of open- angle glaucoma and afflicts more men than women. In most cases, it manifests in the twenties and thirties, threatening lifelong vision impairment. This type of glaucoma typically afflicts myopic or nearsighted people; the structure of the eyes appears to play a significant role in the development of pigmentary glaucoma. Myopic eyes have a concave-shaped iris, which creates an abnormally wide angle. When this happens, the layer of eye pigment rubs on the lens. The rubbing causes the pigment of the iris to mix into the aqueous humour and come into contact with the nearby eye structures like the trabecular network. When the pigment clogs the pores of the meshwork, the IOP rises. Miotic therapy is the most popular treatment but the medications in the form of drops can cause vision blurring in younger people. Laser iridotomy is being tested as an alternative treatment.
Exfoliation Syndrome This is a common form of glaucoma found everywhere in the world but is most prevalent amongst people of European lineage. In about one-tenth of people above 50 years of age, a whitish material builds up on the lens. This exfoliation material looks like tiny flakes of dandruff in a slit-lamp examination. It is rubbed off the lens by the motion of the iris, when pigment is also rubbed off the iris. The rubbed-off exfoliation material and the pigment clog the trabecular meshwork raising the IOP, sometimes to dangerously high levels. Exfoliation syndrome can lead to open-angle glaucoma as well as angle-closure glaucoma, often in the same person. However not all patients with exfoliation syndrome develop glaucoma, but the chances of being afflicted by glaucoma become six times higher. For reasons not known, it often appears in one only eye long before the other is affected. If a patient has glaucoma in one eye, that is probably where she/he is headed. Exfoliation syndrome can be detected before glaucoma ‘attacks’. Patients can be observed more closely and the chances of vision loss can be minimized.
Trauma-Related Glaucoma Any injury to the eye, either a direct blow, chemical burns or a penetrating injury may lead to the development of acute or chronic glaucoma. Glaucoma can set in due to a physical alteration or a mechanical disruption of the eye’s drainage system. Hence, it is crucial for anyone who has suffered eye injury to have regular eye check-ups.
Who is at Risk? Glaucoma can afflict any human being with an eye, and it can be due to various reasons as seen above. Early detection and treatment of glaucoma are the best way to preserve vision. Consequently, the importance of regular eye examination for people of all ages cannot be over- emphasised. However, there are some conditions associated with the disease that puts some people at greater risk of developing glaucoma: �People over 45: Though younger people are not immune to glaucoma, older people have a greater tendency to develop the disease �Family History: Glaucoma appears to be a hereditary disease. The tendency to develop the disease may be in the genes. However, it is also true that just because someone in the family has glaucoma, it does not mean others will develop it too.
Who is at Risk? � High Intra-Ocular Pressure: Elevated IOP levels are the most important factor in the development of glaucoma �African Ancestry: People of African descent have a greater tendency to develop primary open-angle glaucoma than people of other ethnicities. �Others: Myopic people, diabetics, long-term steroid/cortisone users and people with an eye injury are more prone to developing glaucoma.
Diagnosing Glaucoma There are a variety of diagnostic tools to determine the presence or absence of glaucoma even when there are no symptoms. Here is a brief description of the tools and how they are used: �Tonometer: A tonometer measures eye pressure. In a procedure known as applanation tonometry, local anaesthesia is administered with eye drops. Then the patient sits at a slit-lamp where a plastic prism is gently pushed against the eye to measure IOP. Air tonometry is an investigation, in which a puff of air is directed onto the cornea to measure IOP. No anaesthesia is required here, as the instrument does not come into eye contact. �Visual Field Test: A visual field vision tells your eye doctor if and to what extent glaucoma has affected your range of vision. The visual field test is an important indicator of the extent of damage high IOP has inflicted on the optic nerve. There are various field tests a patient may be subjected to. In a computerised visual field test, the patient’s chin is placed on a stand attached to a computerised screen.
Diagnosing Glaucoma Whenever the patient sees a flash of light, she/he is asked to press a button and the doctor takes a printout of your field vision. The Goldmann perimeter test is similar, but no computer is used. The examiner notes down whenever the patient indicates that the light is visible. �Opthalmoscopy: The examiner can look directly at the optic nerve through the pupil with an ophthalmoscope. The appearance and colour of the optic nerve shows whether damage is there and to what extent.
Treating Glaucoma The purpose of treating glaucoma is to prevent further loss of vision because it is irreversible. A number of treatment methods are used depending on the patient’s condition. Treatments can range from simple medications like eye drop and pills to laser surgeries and eye operations. A combination of the above methods may also be used. The key to prevent vision from deteriorating is keeping IOP levels under control. Eye drops may cause a burning sensation at first due to the antibacterial substance present in the medicine. However, the discomfort lasts for only a few seconds. It is vital that the drops be administered exactly as prescribed if the IOP level is to be kept low. Some drops with a ‘duration of action’ of six hours may be prescribed four times a day, to keep the drug effective for 24 hours. Eye drops are absorbed into the bloodstream so it is important to keep your doctor informed of other medications you may be taking.
Treating Glaucoma Patients can minimise the absorption of drugs into the bloodstream and maximise the amount absorbed into the eye. They can do this by closing their eyes for one to two minutes after the administration of the drops and press gently against the nasal corner of the eyelids. The latter procedure closes the tear duct that drains into the nasal cavity
To Know More Let's Connect www.nelivigieyehospital.com Also Follow Us On LinkedIn YouTube Instagram Facebook @nelivigieyehospital