Download

1 / 46
460 likes | 547 Views
Hypersensitivity reactions. marshnes@yahoo.com. Figure 1-32. Immune responses. Hypersensitivity Reactions. Harmful immune responses against harmless ‘environmental’ antigens (pollens, food, drugs)

E N D
Hypersensitivity reactions marshnes@yahoo.com
Figure 1-32 Immune responses
Hypersensitivity Reactions • Harmful immune responses against harmless ‘environmental’ antigens (pollens, food, drugs) • Classified into 4 type of reactions (Coombs & Gell), based on their effector mechanisms responsible for cell & tissue injuries
Classification Allergy has many faces Antibody/B cell- mediated allergy
Classification (contn’d) T cell-mediated Allergy
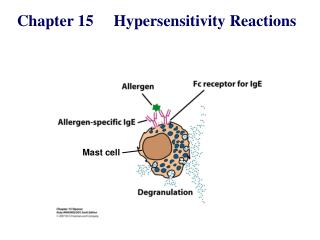
Type I Hypersensitivity reactions(immediate type)* Allergy the commonest type* IgE-mediated* Innocuous antigens: allergens
IgE antibodies • Mediate mast cell activation degranulation • Via their Fce that interact to FceRI with high affinity cytophilic (reaginic) Ab • Normal serum concentration: less than 1 mg/mL • Can rise to over 1000g/mL in severe atopy and helminthic infections • Has totally 5 Ig domains (4 constant and 1 variable heavy chains)
FceR • Fce R I • A high affinity receptor • Mast cells, basophils, activated eosinophils • Fce R II (CD23) • A low affinity receptor • B cells, activated T cells, monocytes, eos, platelets
Binding of IgE into its corresponding receptor: IgE-like domains of a-chain Mediate signal transduction
The nature of allergens • High soluble proteins • Presented to immune system: at very low doses • Enzymes frequently triggers allergy • Cysteine protease of house dust mite(Der p 1) • Phospholipase A2 in bee venom • Others: pollen, mold spores, latex, certain drug, ie. penicillin
Enzyme triggers allergy of the airway Dermatophagoides pteronyssimus Cysteine protease Der p 1
The role of protease & protease-activated receptors (PARs) • Principles • Extracellular exo-and endogenous protease (mites, molds) react with cell-surface receptor leukocyte infiltration, amplify allergic responses • PARs • 7-transmembrane proteins coupled to G proteins: PAR-1,2,3 and 4. PAR-2 is the most important • Expressed on the cells involved in allergic rhinitis and asthma: epithelium, mast cells, eosinophils, neutrophils, monocytes-macrophages, lymphocytes, smooth muscle, endothelium, fibroblasts, neurons
PAR stimulation • Increased intracell. Ca++, gene transcription • Epith.: opens tight junction, desquamation, produces cytokine, growth factors • Degranulates eosinophils, mast cells • Fibroblast: promotes proliferation, maturation, increase collagen prod. • Amplify IgE production • Bronchial muscle: contraction, proliferation • Trypsin (injured epith. cells), tryptase (mast cells)activ. PAR-2 • Chymase (mast cells) activ. PAR-2
Factors leading to IgE production • Two main signals • Polarization into Th2 phenotype • IL-4, IL-5, IL-9, IL-13 • Stimulate IgE switch by B cells • IL-4, IL-13
Contribution of genesand environmental factors Hygiene hypothesis (1989) Infections in early childhood Th1 response Non atopic
Positive interaction between infection and development of atopy RSV infection bronchiolitis Th2 cytokine production: IL-4 (away from IFN-g)
New theory: Immunoregulatory disorders • Modern living reducing contact with pathogens that prime Th1 response (1989) • Modern living conditions defective maturation of Treg and APCreg
The changes of theory? • Clinical evidence • Simultaneous autoimmunity-and IBD (Th1-mediated), and allergies (Th2-mediated) • Crucial factor: Teffector/Treg balance • Absence of immunoregulation develop Th1 or Th2-mediated inflammatory disorders • Depending on own Th1/Th2 bias, genetic background, immunological history
The ‘old friends’ hypothesis • Harmless microorganisms (helminths, saprophytic mycobacteria, lactobacilli) • Less contact with ‘old friends’ in modern living • Allergy: less frequent in hookworm n schistosomiasis • Less lactobacilli in the guts of children allergy; high doses of lactobacilli inhibits dev. of atopic eczema • M.vaccae maturation of Treg treat pre-existing allergy
modification of the hygiene hypothesis • “counter-regulation hypothesis”
“Counter-regulation hypothesis” • All types of infection • Produce IL-10, TGF-b down regulate Th1 n Th2 responses • PAMP TLRs of DC • LPS TLR-4, CpG DNA TLR-9, IFN-g indoleamine 2,3-dioxygenase (IDO) • DC IDO T reg suppress Th2-driven inflammation
Regulatory T cells (T reg) • Natural T reg (CD4CD25) • Defective in atopy (no suppression of Th2 cytokine production) • Defective in FoxP3 allergy, hyper IgE, airway inflammation
CD4 Th17 Allergy/inflammation • IL-17
Role of mast cells • Effector cells of immediate hypersensitivity • Contain cytoplasmic granules, whose contents are the major mediators of allergic reaction • Vasoactive amines, lipid mediators, cytokines • Two subpopulations are detected • Connective tissue (CTMC) and mucosal (MMC) • Specific locations within the tissues • Close to blood vessels, nerve, smooth muscles
Eosinophils • Reside in the connective tissue • Respiratory, gut, urogenital • Toxic granule proteins, radicals parasites • Chemical mediators • Prostaglandins, leukotrienes, cytokines inflammation • Chemokines • CXCL 8, Eotaxins: CCL11, CCL24, CCL26
Toxic proteins and inflammatory mediators of eosinophils , eotaxins
Sequence of events in allergic reaction • Initial exposure of antigen/allergen • Sampling by APC processing & presentation • Stimulation of CD4+T cells Th2 • IL-4 promotes B cells IgE AFC • Sensitization of mast cells degranulation • Immediate/early vascular & muscular changes • vascular permeability & vasodilatation, visceral and bronchial smooth muscle contraction • Late phase reactions, due to proinflammatory cytokines/chemokines • Infiltration & activation of inflammatory cells: eosinophils, basophils, neutrophils
Hypersensitivity in the gut • Food allergy • Celiac disease (gluten-sensitive enteropathy) • a-gliadin • Inflammatory bowel disease (IBD) autoimmune-based inflammatory reactions • overresponsiveness to commensal bacteria
Concluding remarks • Contributing factors to type I hypersensitivity reactions • Allergens • Proteins/molecules-bound to protein, low MW, low dose, enzymatically active, highly soluble • Combination of genetic and environmental factors • CD4+ Th cells, esp. Th2 responses • IL-4 and IL-13 cytokine production IgE switch factor • IgE (cytophilic) antibodies • Mast cells • FceRI