Download
1 / 29
440 likes | 1.56k Views
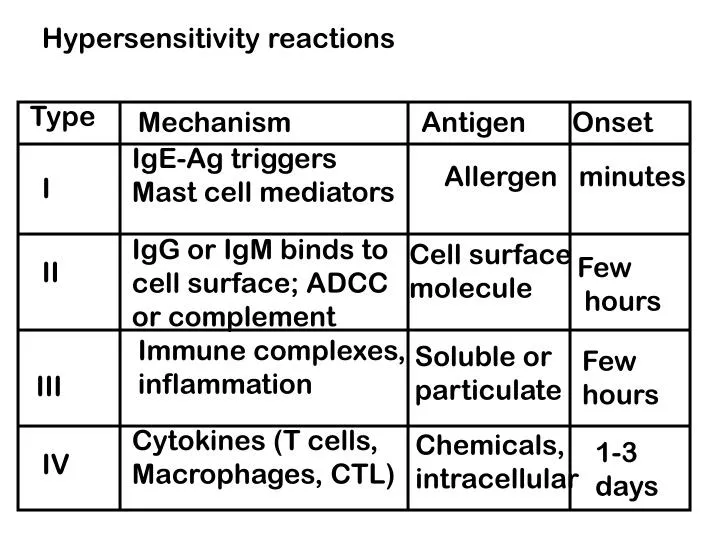
Hypersensitivity reactions. Type. Mechanism. Antigen. Onset. IgE-Ag triggers Mast cell mediators. Allergen minutes. I. IgG or IgM binds to cell surface; ADCC or complement. Cell surface molecule. Few hours. II. Immune complexes, inflammation. Soluble or particulate. Few

E N D
Hypersensitivity reactions Type Mechanism Antigen Onset IgE-Ag triggers Mast cell mediators Allergen minutes I IgG or IgM binds to cell surface; ADCC or complement Cell surface molecule Few hours II Immune complexes, inflammation Soluble or particulate Few hours III Cytokines (T cells, Macrophages, CTL) Chemicals, intracellular 1-3 days IV
Atopy- hereditary predisposition toward allergic reactions Mechanism not clear- may map to chromosomal region encoding many cytokines Tend to occur on mucous membranes- allergens either inhaled or ingested
IgE discovered by Ishizakas in 1960s- normally very rare in serum Larger molecule than IgG Not stable in serum Binds to receptors on basophils and mast cells; then is stable for several weeks
What are mast cells and basophils? Basophil- rare blood cell Mast cells- found in connective tissue Granules contain active mediators Also secrete lots of cytokines: IL-1, IL-4, IL-5, IL-6, GM-CSF, etc. Also have high- and low-affinity receptors for IgE
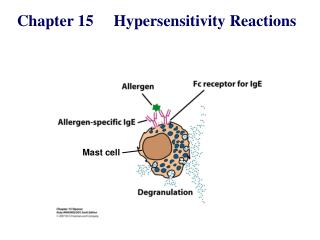
Events in an allergic reaction First exposure B cells produce allergen-specific IgE IgE reacts with Fc receptors on mast cells
Early events required for degranulation Histamine is preformed p. 369
Histamine release occurs within minutes Binds to receptors on target cells smooth muscles contract eosinophils attracted mucus secretion platelet activation blood vessel dilation Blocked by various compounds: antihistamines, Epinephrine, corticosteroids
Effects of type I reactions Systemic anaphylaxis Respiration becomes difficult Blood pressure drops Smooth muscles of bladder and GI tract contract Bronchoconstriction Countered by epinephrine relaxes smooth muscles decreases vascular permeability improves cardiac output
Localized anaphylaxis Allergic rhinitis (hay fever)- nasal mucosa Asthma- lower respiratory tract bronchoconstriction, edema, mucus, inflammation
Early response- histamine, leukotrienes, prostaglandins bronchoconstriction, vasodilation, smooth muscle contraction Late response- IL-4, TNF-, etc. endothelial cell adhesion Also leukocyte migration, leukocyte activation factors Neutrophils (also eosinophils) cause a lot of tissue damage
Food allergies cells are sensitized in GI tract if bloodborne, can cause symptoms such as asthma or hives Atopic dematitis (eczema) Late-phase reactions (not asthmatic) mast cells release cytokines eosinophils, neutrophils recruited
Regulation of type 1 hypersensitivity Antigen stimulation IL-4 induced class switch TH2 cells, also mast cells IFN- reduces IgE production
Detection of type I hypersensitivity (p. 375) RIST- total serum IgE RAST- IgE specific for a single allergen Skin test
Therapies Avoidance Hyposensitization Drugs antihistamines (block receptors) epinephrine (maintain high cAMP and prevent degranulation cromolyn sodium block calcium flux and more (p. 377)
Type II: antibody-mediated cytotoxic reactions Antibodies bind to cells and mediate their destruction Transfusion reactions (ABO blood group Ags) Drug-induced hemolytic anemia drugs absorb to RBCs, like hapten-carrier
p. 415 p. 380
Type III: Immune complex disease Sometimes antibody- (soluble) antigen complexes are not cleared like they should be When deposited in tissue, they cause damage complement activation- produces inflammatory mediators neutrophils Arthus reaction- sensitized person develops a reaction at site of exposure (slower than type I)
Generalized reaction- large amounts of antigen enter bloodstream Immune complexes form Serum sickness- immunization with foreign serum Complexes tend to accumulate in kidneys, arteries, joints Autoimmune disease Infectious disease (malaria, parasitic disease) Cross-reactivity with bacterial or viral antigens
Type IV (TDTH and TC, or delayed-type) Can lead to granuloma formation Detected with skin test (e.g., skin test for tuberculosis) Contact dermatitis- when small molecules complex with skin proteins Internalized and presented by Langerhans cells TH1 response; elicitation of macrophages
Helps protect against intracellular pathogens Granulomas form in chronic reactions DTH response declines in immune deficient people (with T cell deficiency)