Download
1 / 31
310 likes | 464 Views
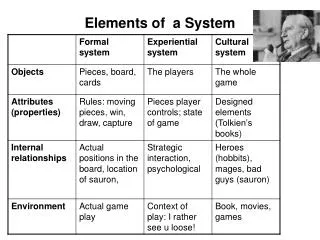
ELEMENTS OF A CLINICAL HISTORY. The sacred seven Helen Murphy RT(R). Localization. This is defined as the exact area of the patient’s complaint. *Ask: Where does it hurt, could you point to it for me? * left or right, anterior or posterior, medial or lateral, upper or lower

E N D
ELEMENTS OF A CLINICAL HISTORY The sacred seven Helen Murphy RT(R)
Localization • This is defined as the exact area of the patient’s complaint. *Ask: Where does it hurt, could you point to it for me? * left or right, anterior or posterior, medial or lateral, upper or lower *name the part: ankle, hand, finger etc.. *Write : Posterior upper neck pain.
Chronology • The arrangement of events in time. *Ask : when did this happen? *Write: Stiff neck and decreased range of motion after motor vehicle accident three days ago. * write date out 28 September 2011
Quality This describes the character of symptoms. * chronic, acute, throbbing, sharp, dull, aching, burning, radiation, pressure. *Ask: What does it feel like? *Write : Sharp pain down both arms.
Severity • This describes the intensity, quantity or extensiveness of the problem. * Ask : On a scale of one to ten how would you rate your pain? * pain rating was a ten but post medications it’s now a four.
Onset • This relates to when the symptoms began and/or what the patient was doing at the time the symptoms began. * Ask : What were you doing when this happen? * Write: Sudden onset headache with no known injury.
Aggravating or alleviating factors • Circumstances that intensify or diminish the condition. *Ask: Does anything make the pain better or worse?
Aggravating or alleviating factors * Write: Pain greater with flexion and extension. * Write: Headache is greater when lights are on.
Associated Manifestations What, if any, symptoms accompany the chief complaint. *Write: Posterior upper neck pain with right arm numbness when patient raises arms above head. *Write: Nausea and vomiting when upright.
History: for c-spine Posterior upper neck pain. Motor vehicle accident three days ago now has stiff neck and decreased range of motion. Sharp pain down both arms with numbness. Pain rating was a ten but post medication it’s now a four. Pain greater with flexion and extension.
Two reasons we need a good HX First the radiologist depends on the clinical histories that we provide to aid in the interpretations. We see the patients they do not!
Helen, FYI for students: Please see the note below from Dr McCabe. This is the same information we provided on the requisitions in the past, just in the online form now. The more information we can supply the better! Karen A large percentage of fluoro studies of the spine that are read by the neuro section are missing either the fluoro time, the contrast amount, or both. The most commonly involved studies are the facet joint and epidural injections. This causes delays in dictating and more work for everyone involved. I would like to start having the fluoro tech fill out both of these sections in the online form (OLF). If there is no contrast used, then a '0' or 'none' would be placed in the text box. By consistently filling out both boxes, the hope is that there will be less wasted time and subsequent production loss. Thank you for your attention to this matter. Please respond with any questions or concerns. Ken McCabe Helen, FYI for students: Please see the note below from Dr Lewis. Karen We are still getting crap for histories on the OLF’s. The point of the OLF is to have a meaningful history, properly spelled and grammatically correct so it can be dropped into the report as written on the form. This never happens from SHMC, particularly from the ICU portables. ‘Patient is on a ventilator’ is not a billable history. SHMC is throwing money down the toilet if we choose to use this history and/or decreasing our efficiency by making us come up with some plausible history on studies if we choose not to use the junk provided. Dr Lewis
Second we also need it to bill the patient correctly so we will get full reimbursement from the insurance companies.
Places to find a HX • Inpatient • * in the chart • - H&P • - Progress notes • - Docotor’s orders
Past medical history or history and physical ( H&P) This is a form that must be in the patients chart before entering a procedure/OR room (H&P can’t be more then 30 days old)
Progress note: The Dr and/or nurse may make notes regarding the patient's condition and onset or continuation of symptoms.
DOCTOR’S ORDERS This will have the exam order and sometimes a history.
Out patient *Check the order for history. *You might have to ask patient for more history then what is given.
ER patients *There is no chart with this patient. *There sometimes is no written order with the patient.( SHMC pink slip with patients but you can’t read them) * Check Meditech *It is up to you to make sure you are doing the correct exam. *Talk to ER doctor.
Symptoms VS Diagnosis The symptoms that a patient is exhibiting or complaining of may not match the original diagnosis.
Reasons for Exams Finding the reason for an exam may be more difficult for some exams than others.
Reasons for a CXR • Chest pain • Shortness of breath (SOB) • Cough • Fever • History of cancer (Ca) • History of stroke • COPD (chronic obstructive pulmonary disease) • CAD (coronary artery disease) • History of smoking • Prior History of heart or lung problems (high blood pressure) • Diabetes • Renal failure • Pre-Operative
? To ask CXR patient: • Do you smoke? • Do you have any difficulty breathing? • Are you ever short of breath? • Have you had pneumonia? • Do you have emphysema or asthma? • Have you had a cold, the flu, a fever or sinus infection recently? When?
Confidentiality • Here we go again!!!! • Medical information is confidential • Do we need to know all the patient health information (HIPAA)?
The bare minimum The very least that you need to have if all else fails is the patients symptoms and how long they have been present. Short of breath for the last three days.