Download
1 / 21
220 likes | 540 Views
Thyroid Debate (Papillary Thyroid Cancer: Extent of Thyroidectomy) . 30 Aug 2007 Surgery-OMMC. JGGuerra, MD HCruz, MD. Papillary Thyroid Cancer: Controversies in treatment.

E N D
Thyroid Debate (Papillary Thyroid Cancer: Extent of Thyroidectomy) 30 Aug 2007 Surgery-OMMC JGGuerra, MD HCruz, MD
Papillary Thyroid Cancer: Controversies in treatment • Surgical resection is the key to management of thyroid cancer, but determining the optimal surgical procedure for individual cases has been controversial.
A prospective, randomized study of total vs less than total thyroidectomy is impossible • due to the excellent outcome in the low-risk group • the requirement of long-term follow-up • large number of patients needed to show any statistical difference in long-term survival outcome.
Management protocols for WDTC are based on retrospective data on prognostic indicators (patient risk and tumor risk factors) • Clinicians rely on large patient cohort studies in which therapyhas not been randomized, leading to some disagreement aboutmanagement
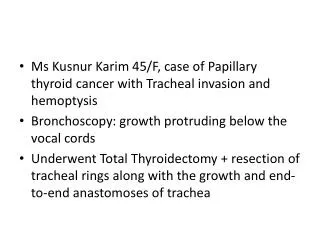
It is timely to discuss whether total thyroidectomy is a better treatment option compared to subtotal thyroidectomy for a 45F with 2 cm papillary thyroid cancer
Premise Is total thyroidectomy a rational treatment of choice for a 45F with 2cm papillary thyroid cancer? YES
Arguments • 30%-87.5% of papillary carcinomas involve opposite lobe (Hirabayashi, 1961, Russell, 1983) • 10%-20% develop recurrence in the contralateral lobe (Soh, 1996) • Lower recurrence rates, some studies show increased survival (Mazzaferri, 1991) • Facilitates earlier detection and tx for recurrent or metastatic carcinoma with RAI (Soh, 1996) • Residual WDTC has the potential to dedifferentiate to ATC
Databank: Total Thyroidectomy • Analysis of surgical procedures performedin over 1500 United States hospitals reveals that among 5584patients with thyroid cancer the majority (77.4%) underwenttotal thyroidectomy regardless of tumor histology and stage (Mazzafferi)
Recurrence rates with lobectomy • Performing lobectomy alone may result in a 5–10%recurrencerate in the opposite thyroid lobe (4,1), a high tumor recurrencerate, and a high (11%) incidence of subsequent pulmonarymetastases.
Multicentricity • The fact that local recurrence signifies a substantial risk of subsequent tumour-related mortality is emphasized by several workers • Total thyroidectomy eliminates the multicentric microscopic foci present in up to 85% of papillary carcinomas6,12 as potential sites of local recurrence, or the anaplastic transformation that occurs in 1%3
Patients undergoing lobectomy have a recurrence rate in the contralateral lobe of 5 to 25%, with a mean of 7%, and up to one- half of these patients eventually die of thyroid cancer, some of whom were initially considered low risk.5
Cancer mortality rates with lobectomy • Hay et al.reported that patients treated for low-risk papillary cancers[Age, Grade, Extent, Size (AGES) score 3.99] had no improvementin survival rates after undergoing more than lobectomy. • Later,they reported the results of a study designed to compare outcomesafter unilateral or bilateral lobectomy for papillary cancer consideredto be low risk by AMES criteria.
Although there were nosignificant differences in cancer-specific mortality or distantmetastasis rates between the two groups, the 20-yr rates forlocal recurrence and nodal metastasis after unilateral lobectomywere 14% and 19%, respectively, significantly higher (P = 0.0001)than the 2% and 6% rates, respectively, seen after bilateralthyroid resection
Hay et al. (30) concluded thatbilateral thyroid resection is the preferable initial surgicalapproach to patients with low-risk papillary cancer
Tollefsen et al reported a 5.7% local recurrence rate in the contralateral thyroid remnant, and 41% of these patients died.
Summary • Retrospective data showed favorable result for total thyroidectomy in terms of • low recurrence rate in the ipsilateral lobe • prevention of development of cancer on the contralateral lobe • acceptable morbidity • facilitation of post operative treatment
References • Clark OH. Total thyroidectomy: the treatment of choice for patients with differentiated thyroid cancer. Ann Surg1982; 196: 361—70 • Hay ID, Grant CS, Taylor WF, McConahey WM. Ipsilaterallobectomy versus bilateral lobar resection in papillary thyroid carcinoma: a retrospective analysis of surgical outcome using a novel prognostic scoring system. Surgery 1987; 102: 1088—95. • Grant CS, Hay ID, Gough IR, Bergitralb EL, Goellner JR, McConahey WM. Local recurrence in papillary thyroid carcinoma: is the extent of surgical resection important? Surgery 1988; 104: 954—62 • Mazzaferri EL, Young RL. Papillary thyroid carcinoma: a 10-year follow-up report of the impact of treatment in 576 patients. Am J Med 1981; 70: 511—8.
5. McConahey WM, Hay ID, Woolner LB, van Heerden JA, Taylor WE. Papillary thyroid cancer treated at the Mayo Clinic, 1946 through 1970:initial manifestations, pathologic findings, therapy and outcome. Mayo Clin Proc 1986; 6: 978—96. 6. Rossi RL, Cady B, Silverman, ML, Wool MS, Homer TA. Current results of conservative surgery for differentiated thyroid carcinoma. World JSurg1986; 10: 612—22. 7. Shah JP, Loree TR, Dharker D, Strong EW. Lobectomy versus total thyroidectomy for differentiated carcinoma of the thyroid: a marched-pair analysis. AmJSurg1993; 166:331—5. 8. Tollefsen HR, Shah, JP, Huvos AG. Papillary carcinoma of the thyroid. Recurrence in the gland after initial surgical treatment. AmJSurg1972;124: 468—72.