Download
1 / 36
360 likes | 370 Views
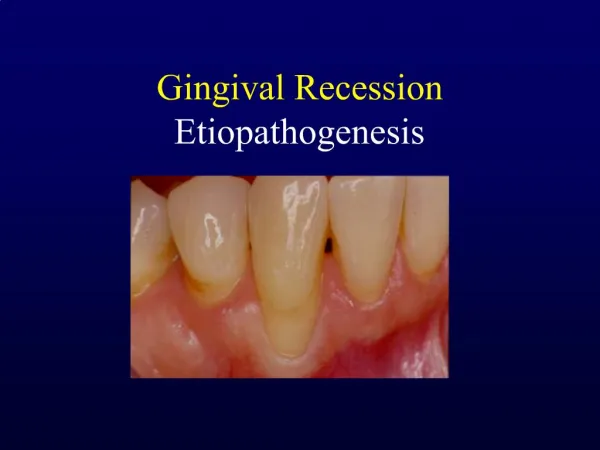
Gingival Tissue Management. V ery often when caries extend subgingivally , preparation, isolation and restoration of the area becomes difficult. Also restorations placed here can impinge on gingival tissues.

E N D
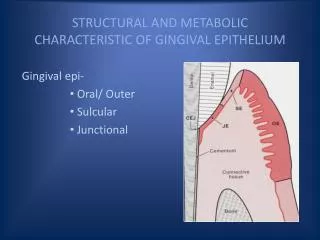
Very often when caries extend subgingivally, preparation, isolation and restoration of the area becomes difficult. Also restorations placed here can impinge on gingival tissues. Gingival tissue is very sensitive to foreign materials. Proximity of restorations to gingiva can cause gingival inflammation, plaque retention and eventually periodontal disease. Since a sound periodontium is the foundation for good restorative treatment, it is necessary to manage the gingival tissues prior to the restoration. This also helps in achieving maximum possible properties of the restorative material and in ensuring longevity of the restoration
Gingival tissue management can be described as, the procedure of temporary eversion or resection of gingiva away from the tooth surface or deepening of gingival sulcus to expose the cervical portion of tooth in order to have proper marginal finish to the restoration and for establishing a good cervical cavosurface margin for the tooth preparation or for recording the preparation accurately. The procedure of exposing gingival finish lines of a tooth preparation may be termed as gingival displacement, gingival retraction or gingival tissue deflection
Indications: Caries/cavity margins extending subgingivally Control gingival hemorrhage or fluid flow Esthetics Enhancing retention Recording of preparation margins in impression Removal of gingival overgrowth
Physicomechanical methods: - Mechanically displaces free gingiva apically & laterally away from preparation margins - Employed only when gingiva is healthy and have a definite zone of attached gingiva apical to the free gingiva. Adequate bone support with no signs of resorptionshd be present. - Provides minimal retraction Various methods employed are: Rubber dam, rolled cotton or synthetic cords, wedges etc
Rubber dam: Heavy gauge rubber dam is used for adequate gingival displacement. For extra retraction, cervical clamp can be used. Adv: Immediate results Disadvantages: Full arch impressions are difficult with this technique.
Wedges: Used interproximally to depress gingiva. Care shd be taken not to insert it forcefully Rolled Cotton Twills: Cotton can be rolled and mechanically packed into gingival sulcus. These twills can also be used by rolling it in fast setting ZOE. After drying, it is placed in gingival sulcus. It should remain in place for 48 hrs to be effective. Longer period can cause loss of periodontal attachment.
Copper band: A copper band is welded to form a tube corresponding to the size of prepared tooth. One end of the tube is trimmed to follow the profile of gingival finish line. After positioning & contouring the tube over the prepared tooth, it is filled with impression material. Impression material will displace gingiva exposing the finish line. Disadv: Time consuming, sharp margins can injure gingival tissues
Retraction cords: Can be made of cotton or synthetic fibers; may be braided or non braided. Some cords have metallic or resin wire wrapped around them to assure their compactness, immobility and non shredding. Cords are available in sizes 000, 00, 0, 1, 2 and 3 and are colour coded. They may be plain or impregnated with chemicals.
Plain cords can be mechanically forced gently into gingival sulcus. They not only aid in isolation against gingival fluid but also produce gingival deflection. Disadv: Can cause injury to gingival tissues and initiate bleeding
Chemicomechanical methods: This is a method of combining a chemical with pressure packing. Retraction cords, drawn cotton rolls or cotton pellets impregnated with chemicals are used for stoppage of bleeding and seeping of crevicular fluid. Chemicals used can be of 3 types: Vasoconstrictors Biologic fluid coagulants/Astringents Surface layer tissue coagulants
Due to its looseness, impregnated cotton rolls can be easily placed than cords. But the disadvantage is that part of the coagulated sealing layer on the sulcus wall may get incorporated within the cotton. When the cotton is removed, the coagulated membrane may get peeled off initiating bleeding and fluid seepage which may be vigorous than before. Cords may be supplied impregnated with the chemical or the chemical may be added before insertion of the cord or after insertion while the cord is in the sulcus.
Technique for placement of retraction cord - The operating area shd be dried - Select the appropriate sized cord. Measure the tooth diameter before cutting the cord. Cord slightly longer than the length of the gingival margin shd be precut. Excess may lead to displacement of already packed portions. - Cord can be dipped in 25% aluminum chloride (Hemodentlqd) in a dapen dish to control hemorrhage. Excess lqd is removed by squeezing the cord using cotton sponges
- The cord is packed with appropriate instruments called cord packers that are shaped like blunt hatchets or hoes, preferably with serrations. Cord packers are available in various sizes to accommodate different locations. - Start packing from the mesial surface of the tooth, going systematically to the other end making sure that the packed part is stable before packing the next part.
- During packing, gentle force is applied in a mesial and lateral direction so that the packed cord doesn’t get dislodged. Avoid applying apical pressure as it may harm the junctional epithelium It is emphasized that the cord is placed to widen the sulcus and not to depress soft tissue gingivally - When the free gingiva is thin and the sulcus is narrow, a cord of very narrow diameter is placed. When the gingival margin is deep, it is helpful to insert a second cord of same or larger diameter over the first to keep the sulcus from narrowing at the gingival crest. - Avoid putting the ends of the cord interproximally . The ideal location is at the axial angles of the tooth where interdentalcol has maximum height for better gripping and stabilization of the cord
- Hemorrhage or seepage during insertion of the cord can be controlled if an assistant repeatedly touches the cord with dry cotton or dries the area with a gentle steam of air. If there is excessive bleeding a cotton pellet dipped in aluminum chloride is pressed on the tissue for 5 min before reinserting the cord. - The cord shd remain in place for at least 5 min. If hemorrhage or excessive tissue is present, a minimum of 10 min is recommended. - The region must remain dry during this period and the patient shd be cautioned not to close the mouth or allow the tongue to stray on the teeth. - Removal of the packed material shd be done gently & in a hydrous field so that the moisture will act as a lubricant between the cord and the sealing film. Disturbing this film can initiate bleeding.
- Inspect the region. After proper retraction, the soft tissue shd be standing away from the tooth, clearly exposing the gingival margin. Any corrections in the gingival aspect of the cavity preparation/ tooth preparation can be done now. Re inserting after this step which will be easy and rapid
Chemical methods: - This is one of the oldest method used for retraction of gingiva. - Caustic chemicals like sulfuric acid, trichloracetic acid, negatol( combination of metacresolsulfonic acid & formaldehyde) etc are used to chemically cauterize gingival tissues. Method: Blade of a plastic instrument is dipped in the chemical & placed in the gingival margin for 1 min after which it is washed off. It is used where minimum retraction is reqd with control of blood &fluid flow such as during Class V restorations Disadv: Due to their caustic nature and potential for soft tissue injury, except for trichloracetic acid, chemicals are seldom used now
Rotary curettage/Gingittage/Denttage - This is a troughing technique wherein a portion of the epithelium within the sulcus is removed with high speed handpiece and chamfer diamond bur during placement of restorative margins subgingivally Disadv: This technique offers poor tactile sensation Uncontrolled procedure Can potentially damage periodontium Excessive bleeding
Surgical method: - This involves surgical excision of interfering gingival tissue using sharp surgical knife - Used when interfering gingiva has to be removed in case of gingival hypertrophy or extensive tooth fracture extending subgingivally - Temporary restoration is given for 2 wks. Permanent restoration is done after the wound heals during which one of the suitable displacement methods can be adopted
Electrosurgical method: - Also called surgical diathermy - Used esp to manage hypertrophic gingiva that doesn’t respond to conservative periodontal treatment Principle: Uses high frequency alternating current concentrated at tiny electrodes to produce localized changes within tissues which is confined to 2-3 cell layers 4 actions can be produced at the electrode end; Cutting, Coagulation, Fulgeration, Dessication
Cutting: is done precisely using minimum energy. Minimum tissue involved. It doesn’t induce any bleeding Coagulation: Thermal energy causes coagulation of tissues ,their fluids and oozed out blood Fulgeration & Desiccation involves deeper and larger areas and causes carbonization For gingival tissue retraction, cutting and rarely coagulation action is used
Adv: Rapid atraumatic cutting action Sterilizes wound immediately Heals by primary intention without pain, swelling or scarring
Recent techniques: - Lasers - Dilation of gingival sulcus - Stay - put retraction cord
Laser: Nd- YAG lasers are recommended for gingival tissue retraction and excision. Works by photoablation mechanism Adv: Controlled, painless and bloodless tissue removal Rapid healing Disadv: Slow technique Expensive Retraction by dilation of gingival sulcus Several methods are available for achieving gingival retraction through dilation of gingival sulcus Eg: Expasyl, Magic foam, GingiTrac, Merocel strips etc
Magic foam Magic foam consists of expanding polyvinylsiloxane material designed for easy and fast retraction of the sulcus without the potentially traumatic and time consuming packing of retraction cord. It is a non haemostatic cordless retraction system and consists of foam and cartridges, mixing and intraoral tips, comprecaps (3 sizes)
Technique of application of Magic foam - Select Comprecap as per the anatomy of tooth. - Apply Magic FoamCord around the preparation by syringing. - An application in the sulcus is only necessary where there is a deep sub-gingival preparation margin
- Place Comprecap over preparation. And the patient’s is ask to bite down for 3 -5 minutes. This procedure makes optimal use of the formation of foam (i.e., the expansive effect of the silicone foam). Due to the counter pressure of the Comprecap, the expansion of the Magic FoamCord occurs in the sulcus. - After proper setting, remove the Comprecap Anatomic and Magic Foam Cord in one piece.
Adv: Non-traumatic, conservative method of temporary gingival retraction Better patient comfort Easy and fast application Disadv: Hemostasis cannot be achieved. Relatively expensive compared to cord. No improvement in speed or quality of retraction compared with cord Less affective in subgingival margins
Expasyl: This is a paste that contains aluminum chloride and kaolin. It has a specially formulated consistency which exerts moderated calculated pressure on gingiva - Has both mechanical and chemical action. It creates and maintains space in the sulcus due to optimal characteristics of its viscosity which is mainly due to its kaolin component. It achieve hemostasis due to aluminum chloride. Time taken for retraction is 2 minutes and sulcus widening achieved is 0.5mm
Adv: Physically displaces tissue for good marginal access Minimal time and force needed compared with packing cord. Safe minimal pressure required and no danger of rupturing epithelial attachment. Disadv: Expensive Is effective only under specific, limited conditions. The paste's thickness made it difficult for some evaluators to express it into the sulcus. Disposable metal dispenser tips are too large, making it difficult to express Expasyl into the interproximalsulcus
GingiTrac It is a mild natural astringent in gel form. Utilizes patient’s bite pressure to push material into sulcus and retract gingiva. Merocel Strip A synthetic material that is specifically chemically extracted from a biocompatible polymer (hydroxylate polyvinyl acetate) Merocel Strip expands by absorption of oral fluids and exerts pressure on surrounding tissue
Stay put retraction cord: Fine metal filament reinforced displacement cord. It is a unique combination of softly braided retraction cord and ultra fine copper filaments. May be Impregnated/ Non-impregnated. When the stay – put cord is shaped, it remains in shape and does not deform Adv: Can be easily adapted. Can be preformed Does not lift in the sulcus Does not unravel. Can be impregnated with an astringent or haemostatic solution as required
Atraumatic gingival tissue management provides greater patient comfort. During restorative procedures, it is incumbent upon clinicians to consider the advantages and limitations of each method in individual case and patient, and to strive for minimally invasive methods that optimize the procedural site for impression making and restoration placement.