Download
1 / 19
220 likes | 496 Views
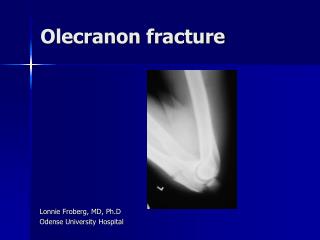
Olecranon Fractures. By: Christine Davis http://www.youtube.com/watch?v=hVc3NQhAw_I&NR=1. Common Mechanism . Falling on flexed elbow when triceps are contracted to help break the fall. Commonly an avulsion fracture Direct blow to elbow Elbow hyperextension.

E N D
Olecranon Fractures By: Christine Davis http://www.youtube.com/watch?v=hVc3NQhAw_I&NR=1
Common Mechanism • Falling on flexed elbow when triceps are contracted to help break the fall. • Commonly an avulsion fracture • Direct blow to elbow • Elbow hyperextension
Classification of Olecranon Fractures • Schatzker Classification Transverse transverse impacted Oblique Comminuted Oblique distal Fracture Dislocation
Treatment Goals • Alignment • Articular restoration • Stability • Relationship between humerus and ulna
Treatment • Closed Reduction and Splint or Cast • Used for non-displaced, stable fractures. • Elbow should be held in 90 degrees flexion for 4 weeks.
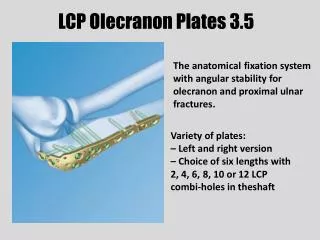
Treatment Cont. • Open Reduction and Internal Fixation (ORIF) • Recommended if less than 45 degrees of flexion is required to maintain reduction • Method of choice for displaced and comminuted fractures • Fixation Methods • Large intramedullary screw • Tension band • K-wires • Plate & screw • Combination
Day One to Week One • Stability: NONE • ROM: • Surgical: Gentle elbow flexion and AROM in wrist • Cast: No ROM to elbow or wrist • Strength: Isometric wrist strengthening in cast after 3-4 days. • Functional Activities: Only one armed activities with uninjured arm.
Week 2 • Stability: None to minimal • ROM: • Surgical: Active elbow flexion and AROM in wrist • Cast: No ROM • Strength: No strength to elbow in extension. Isometric to elbow and wrist. • Functional Activities: Only one armed activities with uninjured arm.
Four to Six Weeks • Stability: Usually stable with bridging callus • ROM: Active ROM in flexion and extension • Strength: Isometric exercises in flexion and extension • Functional Activities: May use affected arm for stability and light self care.
Six to Eight Weeks • Stability: Stable • ROM: Full AROM to AAROM in all planes to elbow and wrist • Strength: Resistive exercise to elbow and wrist • Functional Activities: May use affected arm for everyday activities
Eight to Twelve Weeks • Stability: Stable • ROM: Full AROM and AAROM in all planes to elbow and wrist. • Strength: Resistive exercise to elbow and wrist • Functional Activities: May use injured arm for everyday activities
Expected Time Lost • Expected time of bone healing: • 10-12 weeks • Expected duration of rehab • 10-12 weeks
Muscle Strengthening • Elbow Muscles • Triceps • Biceps • Pronators • Supinators • Wrist Flexors • Flex. Carpi Radialis • Flex. Carpi Ulnaris • Flex. Digitorum longus and sublimis
Muscle Strengthening Cont. • Wrist Extensor • Ext. Carpi Radialis longus and brevis • Ext. Carpi Ulnaris • Ext. Digitorum longus
Rehabilitation Objectives • Restore Elbow ROM • Maintain Shoulder and Wrist ROM
Rehabilitation Objectives Elbow and Forearm ROM Motion Normal Functional • Flexion 150* 90* • Extension -5*-0* lacking 20-30* • Pronation 90* 50* • Supination 90* 50*
Considerations • Check circulation • Check dermatomes • Skin healing problems due to hardware