Download
1 / 37
380 likes | 602 Views
Video Observational Gait Analysis on 5 Dollars a Day. David Webner, MD Associate Director Sports Medicine Fellowship Crozer-Keystone Health System Suburban Philadelphia. References.

E N D
Video Observational Gait Analysis on 5 Dollars a Day David Webner, MD Associate Director Sports Medicine Fellowship Crozer-Keystone Health System Suburban Philadelphia
References • Switaj TL and O’Connor FG: Gait analysis. In Seidenburg PH and Beutler AI (eds.): The Sports Medicine Resource Manual. Philadelphia, Saunders, 2008, pp. 537-42. • O’Connor FG, Hoke B, and Torrance A: Video gait analysis. In O’Connor FG, Wilder RP (eds.): Textbook of Running Medicine. New York, McGraw-Hill, 2001, pp. 59-66. • James SL and Jones DC: Biomechanical aspects of distance running injuries. In Cavanagh (ed.), Biomechanics of Distance Running, Champaign, Ill, Human Kinetics, 1990, pp. 249-69. • Novachek TF: The biomechanics of running and sprinting. In Guten GN (ed.): Running Injuries. Philadelphia, Saunders, 1997, pp. 4-19. • Edington CJ, Frederick EC, Cavanagh PR: Rearfoot motion in distance running. In Cavanagh PR (ed.): Biomechanics of Distance Running, Champaign, Ill, Human Kinetics, 1990, pp. 135-64. • Milliron MJ and Cavanagh PR: Sagittal plane kinematics of the lower extremity during distance running, in Cavanagh PR (ed.): Biomechanics of Distance Running, Champaign, Ill, Human Kinetics, 1990, pp. 65-105
Outline • Background • Recommendations • Fundamentals • Procedure • Equipment • Documentation • Analysis • Examples
Background • History • Initially performed by running coaches in the early 1900s • Reliability increases with experience • Technology • Video-assisted frame by frame • Allows evaluation of non-elite athlete
Background • Research • Predominantly in physical therapy • Rehab patients from CVA • Children with gait abnormalities • CP, neuromuscular disease • No evidence-based research correlating injury with modifications in gait analysis • Athlete variability • Interobserver variability
Evaluation of subtle gait changes not detectable in static examination Orthotic evaluation Gait refinement with limb prostheses Physical therapy Chronic exertional compartment syndrome testing Recommendations
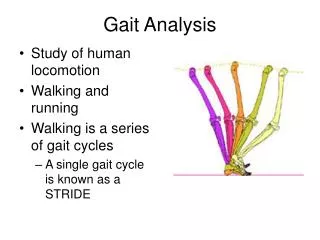
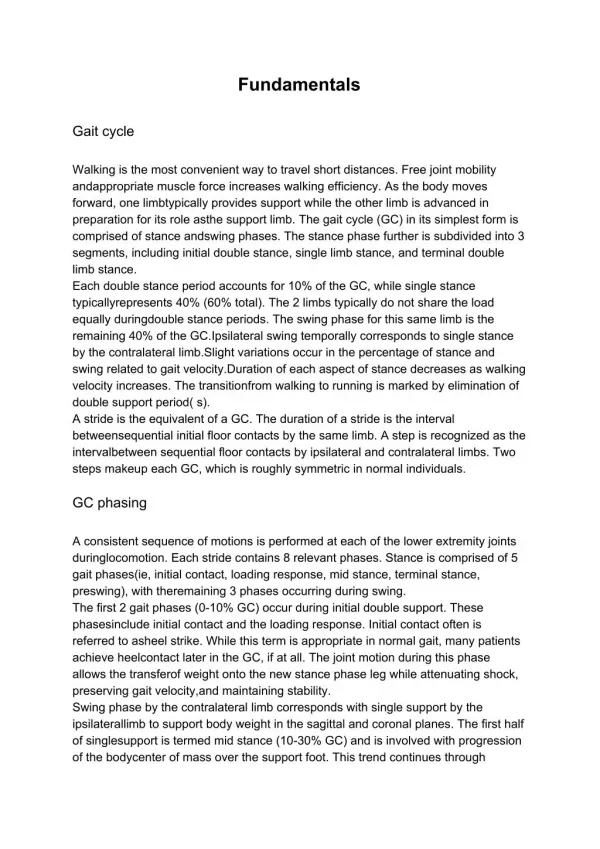
Stance phase (IC TO) Loading response Midstance Terminal stance Preswing Swing phase (TO IC) Initial swing Midswing Terminal swing Fundamentals – Gait Cycle
Walking Stance 60% Swing 40% Double support Running Stance 40% Absorption and propulsion Swing 60% Initial and terminal Double float Fundamentals -- Gait Cycle
Fundamentals -- Definitions • Stride length: • Initial contact of one foot to the other • Depends on height, leg length, skill • Step length: • One complete gait cycle • Cadence: • Number of steps for any given time • Women (6-9 steps/min) > men • Increased speed: • Step length and cadence increase
Kinematics Range of motion of body segments involved in an activity Usually spoken about in the sagittal plane Kinetics Measure of the forces that are responsible for that activity Vertical forces increase from walking to running (1.5 times body weight 4 times body weight) Fundamentals -- Physics
Fundamentals -- Running • Increased speed leads to increased angles • Hips and knees: increased flexion • Increased ankle dorsiflexion • Responsible for lowering the center of gravity
McPoil and Cornwall: Applied sports biomechanics in rehabilitation: running. In Zachazeski, MaGee, and Quillen (eds.): Athletic Injuries and Rehabilitation. Philadelphia, Saunders, 1996, p. 356
Range of Motion • Hip • Increased ROM from walking to running • Increased flexion, and decreased extension • Max extension at take off and max flexion at terminal swing • No coronal plane changes • Pelvis • Initial contact: 8° internal rotation • Take off: 8° external rotation
Walking Initial contact 10° flex 60° (64° flex – 8° ext) Running Initial contact 35° flex 63° (79° flex -16° ext) Flexes during absorption phase while running Midstance: reversal of motion to enter propulsion Range of Motion -- Knee
Walking 18° plantarflex to 12° dorsiflex = 30° total Running Increase to 50° total Increase in hip and knee flexion limit the plantarflexion and produce rapid dorsiflexion in propulsion Range of Motion -- Ankle
Range of Motion -- Foot • Triplanar movement • Pronation = dorsiflexion + abduction and eversion • Supination = plantarflexion + adduction and inversion
Procedure • Systematic process • Prepping the runner • 1 L of miralax • Markers • Prepping your equipment • Make sure the camera’s charged! • Physical Exam • Static stance, shoe wear pattern, upper and lower extremity assessment
Procedure • Sagittal plane • Hip, knee and ankle flexion and extension • Coronal plane • Hip (adduction/abduction) • Knee (varus/valgus) • Foot (inversion/eversion) • Special protocols • Age, speed, incline etc.
2 Hour Gait Analysis • Full physical exam • Static stills shoes off – 4 views • Static stills shoes on – 4 views • Walking shoes off – 4 views • Walking shoes on – 4 views • Running shoes off – 4 views • Running shoes on – 4 views • Review session • Recommendations
30 Minute Gait Analysis • Modified Hoke/Lefever-Button protoccol • Lateral views • Head to feet (30 sec) • Hips to feet (30 sec) • Posterior view • Head to feet (30 sec) • Hips to feet (30 sec) • Knee to feet (30 sec)
Hardware • Exam room • Treadmill • Important extremes too consider • Weight • Speed • Incline • Video camera • Don’t overlook… • Power cord, batteries, videotape • Television/laptop • Be prepared… • Video/audio auxiliary cables • Remote, playback with pause/slow motion features
Documentation • Head • Vertically on shoulders (not to exceed 4 cm) • No anterior/posterior, lateral rotation or side bending • Linearity from ear to shoulder during the entire gait cycle • Elbow • Normal carry is between 80°-110° flexion
Possible Pathology • Head • Abnormalities suggest cervical dysfunction, muscle weakness, or previous cervical trauma • Excessive vertical displacement of the head due to leg length discrepancy • Early heel lift • Shoulder • Abnormal movement may indicate lower extremity injury • Arms crossing the midline • Possibly indicative of pelvic rotation • Wasted running energy
Documentation • Trunk • Should be linear, without flexion, extension or lateral lean • Hip/Pelvis • Pelvic drop should not exceed 4 degrees
Documentation • Knees • Cushioning flexion range: position of the knee at maximum stance flexion minus position at initial contact • Quadriceps weakness with value less than 20° • Swing phase knee flexion less than 115° • Hamstring weakness
Documentation • Ankle • Increased plantarflexion at foot strike • Anterior tibialis weakness • Exertional compartment syndrome (foot drop) • Limited dorsiflexion • Calf tightness • Anterior tibialis impingement • If combined with early heel off… • Plantar fasciitis, metatarsalgia
Documentation • Foot • Normal motion – subtalar joint • Subtalar supination at heel strike, followed by rotation into pronation up to 8° at the end of contact • Repeat supination in midstance, and peaks just before toe off (propulsion) • Early pronation during the swing phase and then in neutral
Measuring Subtalar Motion • Normal motion • 6° of inversion at foot strike • 6-8° of eversion at maximal pronation • Neutral at heel lift • 6-8° of inversion at toe off • Excessive pronation is characterized by persistent eversion
Angle of Gait • Posterior view • Greater than 1.5 inches is too wide-based • Can be indicative of IT band syndrome • External rotation of >7° • Suggests torsional abnormalities • Weak posterior tibial tendon, limited dorsiflexion (?equinus deformity) • Calcaneal whip • Heel rotation on heel rise • Circumduction – lifting of the affected extremity with rotation could be due to weak anterior tibialis, joint restriction or weak hip flexors
Possible Pathology • Trunk • Flexion with running • Weak lumbar stabilizers • Tight hip flexors • Lateral lean (> 4 cm) • Leg length discrepancy • Hip external rotation / abduction weakness • Hips • Excessive external rotation • Tight hip flexors • Weak abductors IT Band Syndrome • Excessive internal rotation • Piriformis