Download
1 / 38
380 likes | 387 Views
CLINICAL CASE. DEPARTMENT FOR IMMUNOCOMPROMISED PATIENTS UNIVERSITY HOSPITAL FOR INFECTIOUS DISEASES “DR. FRAN MIHALJEVIĆ” DIANA DIDOVIĆ, MD PROF. DAVORKA LUKAS, MD, PhD 12 th October 2018. Clinical case. Male patient , 39 years old

E N D
CLINICAL CASE DEPARTMENT FOR IMMUNOCOMPROMISED PATIENTS UNIVERSITY HOSPITAL FOR INFECTIOUS DISEASES “DR. FRAN MIHALJEVIĆ” DIANA DIDOVIĆ, MD PROF. DAVORKA LUKAS, MD, PhD 12th October 2018
Clinical case • Male patient, 39 yearsold • Hospitalized in UHC Zagreb (4th of June – 6th of June 2017) prior to admission to UHID “Dr. Fran Mihaljević” on the 6th of June 2017
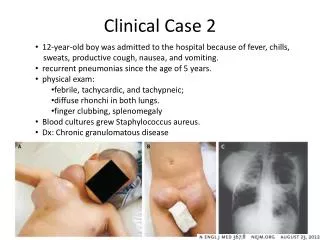
PATIENT HISTORY CURRENT ILLNESS • fever (37,5-38,5°C) usually in the afternoons during the last 20 days • without chills and shivering • night sweats • lost 8 kgs in the last two weeks • fatigue • without respiratory symptoms • three watery stools prior to hospital admission (during peroral co-amoxiclav therapy) • no other symptoms
CURRENT MEDICATIONS • 25th May – 1st June co-amoxiclav 2x1 gr/day • acetaminophen up to 2 gr/day JUST BEFORE CURRENT ILLNESS • healthy PAST MEDICAL HISTORY • acne (puberty) • hidradenitis suppurativa(under therapy for 6 years, last dermatological exam 6 months ago) MEDICATIONS • topical: sucralfate cream and medical soap HABITS • smoking: 20 pack-years • alcohol: occasionally • denies illicit drug use
SOCIAL HISTORY • lives in a house in Dalmatia with his mother • single, has no children • works as a van driver • during the last 6 months occasionally traveled to Split and Zagreb • didn’t travel outside Croatia recently • denies contact with animals and visits to nature • occasionally has unprotected sex VACCINATION STATUS • regularly in childhood; nothing recently ALLERGIES TO MEDICATIONS • none so far
PHYSICAL EXAMINATION AT ADMISSION (UHC ZAGREB) Awake, alert and oriented. Skin is pale. In armpits, neck, back, inguinal and scrotal region skin lesions characteristic for hidradenitis suppurativa. Serous secretion in the right inguinal region. Sclerae are white. Pharynx is pink, without tonsillar swelling or exudates. Without peripheral lymphadenopathy. Carotid pulse 2+ bilaterally without bruit. Lung sounds are clear bilaterally without rales, ronchi or wheezes. Heart rate and rhythm are normal, no murmurs and gallops. Abdomen is soft, bowel sounds are tender and normoactive, without distention, non-tender.Liver present 2 cm below the right costal margin and spleen 4 cm below the left costal margin. Extremities without swelling, arterial pulsations palpable.
LABORATORY RESULTS (UHC ZAGREB) • ESR84, CRP 55,1 • WBC3,1(ne 67,3, ly19,5, mo 6,0, eo 6,6, ba 0,6)% • RBC3,97, HGB102, HCT0,309, MCV77,8, PLT92 • BG5,1, BUN 4,1, SCR 84 • bilirubin6, AST 131, ALT 186, GGT 60, CK 29, LDH 246, ALP 76 • Fe5, UIBC38, TIBC43, ferritin1279,5 • PT0,85, INR1,04, FBG6,5 • Urinalysis: E +++
DIFFERENTIAL DIAGNOSIS? WBC3,1(ne 67,3, ly19,5, mo 6,0, eo 6,6, ba 0,6)% RBC3,97, HGB102, HCT0,309, MCV77,8, PLT92 bilirubin 6, AST 131, ALT 186, GGT 60, CK 29, LDH 246, ALP 76 INFECTIOUS DISEASES MONONUCLEOSIS SYNDROME, BRUCELLOSIS, LEISHMANIASIS, BARTONELLOSIS, HIV INFECTION, TB HEMATOLOGIC DISEASES MYELOPROLIFERATIVE DISORDERS (MDS, AML), LEUKEMIA, LYMPHOMA, MYELOFIBROSIS, SICKLE CELL ANEMIA, THALASSEMIA Hepatosplenomegaly Fever(3 weeks) METABOLIC DISORDERS NIEMANN-PICK DISEASE, GAUCHER DISEASE, HURLER SYNDROME STORAGE DISORDERS AMYLOIDOSIS, SARCOIDOSIS AUTOIMMUNE DISEASE (SLE)
RADIOLOGICAL IMAGING? Chest X-ray: chest radiograph reveals no evidence of active pleural or pulmonary parenchymal abnormality. The cardiac silhouette and mediastinum appear normal. Abdominal ultrasound: liver is enlarged, 16 cm in diameter, hemangioma approximately 4-5 mm in diameter.Gallbladder contracted, spleen is enlarged, measures around 18 cm, homogeneous, splenunculus around 2 cm in diameter. Kidney size and echotexture is normal, without evidence of hydronephrosis. Pancreas is obscured by bowel gas.
FURTHER… • ACE139 • IgG25,89, IgA3,35, IgM1,82 • CEA3,6, CA 12533,7, PSA0,41 • C31,77, C40,25 • ANA (ENA), dsDNA, SS-A, SS-B, DNA-topo 1, Jo-1, CENP-B, ANCA, PR3 ANCA, MPO ANCA –negative • free kappa light chains 53,2, free lambda light chains 48,50
CYTOLOGICAL BONE MARROW PUNCTURE (STERNUM): Myelogram: blasts 1%, promyelocytes 1%, myelocytes and metamyelocytes 15%, unsegmented granulocytes 25%, segmented granulocytes 12%, lymphocytes 13%, monocytes 2%, plasma cells 3%, erythroblasts 28%.Erythrocytes: anisocytosis, polychromasia. Platelets: moderately. Medium abundant hematopoietic tissue is present in bone marrow smears; the ratio of white and red blood cells is 2,5:1. Erythropoiesis is mature and predominantly normoblastic. Granulocytopoiesis is represented by mature and transitional forms. Thrombocytopoiesis is morphologically and numerically within the normal ratio. Numerous phagocytes with blue inclusions are seen in bone marrow smears. Cytomorphologicalfoundings are pathognomonic for infections caused by Leishmaniadonovani.
PHYSICAL EXAMINATION AT ADMISSION (UHID) BP125/70 mmHg, c/p 123/min, RR20/min, SpO2 93% on RA, Ttymp37,3°C Awake, alert, oriented. Pale. Numerous scars on the face, neck and, dominantly, on the back where they coalesce. Hyperpigmented scars located in both inguinal, axillar regions and left leg. A few scabs on the upper lip. Scleraeare white. Pharynx is pink, without tonsillar swelling or exudates. Lymph nodes palpable in the right axillar region. Carotid pulse 2+ bilaterally without bruit. Pulmonary sounds intensified. Heart rate and rhythm are normal, no murmurs and gallops. Abdomen is soft, bowel sounds are tender and normoactive, without distention, non-tender.Liver present 4 cm below the right costal margin and spleen 4 cm below the left costal margin. Extremities without swelling, arterial pulsations palpable. MS negative.
LABORATORY RESULTS AT ADMISSION • Blood type “B”, Rh “+” (positive) • CRP 77,2, WBC 2,0 (ne 71,0, ly 17,5, mo 6,1, eo 4,2, ba 1,2)%, RBC 3,73, HGB 96, HCT 0,287, PLT 79 • BG 6,1 BUN 3,0, SCR 102, Na 140, K 3,8, Cl 105 • bilirubin 7, AST 103, ALT 121, GGT 67, ALP 87, LDH 393, CK 43 • PT 0,69, INR 1,15, APTT 33,9, TT 15,2, FBG 5,4, D-dimers >4,40 • chol 3,1, trig 2,7, HDL 0,4, LDL 1,9 • IgG 20,2, IgM 1,55, IgA 3,09 • TP 77 (alb 42,7, 𝛂1 4,9, 𝛂2 11,2, 𝛃 10,4, 𝛄 30,8)%, A 32,9 g/L, A/G 0,74
Blood culture: sterile. • Urine culture: sterile. • HIV Ag/Ab– POSITIVE • HIV1 RNA307 000 copies/mL(10.6.) • Absolute CD4 lyT count= 8/uL (2.3%) (10.6.) • HLA*B5701 wasn’t detected
Toxoplasma: IgM – negative, IgG - positive 20,2 IU/mL, IgA - negative. • EBV: VCA IgM negative, VCA IgG positive >750, EBV EA negative, EBNA IgG positive 83,5 • CMV: IgM negative, IgG positive • TPHA positive 160, RPR negative • Anti-HAV IgM – negative, HAV Ab total – positive. • HBsAg – negative, Anti-HBs IgG - negative, Anti-HBc total - negative. • Anti-HCV – negative. • Anti-HEV IgM and IgG - negative. • Quantiferontest – negative. • CRAG –negative.
L-AMB* • five doses • 4 mg/kg/day PROPHYLAXIS (MAC, PCP) Abacavir/lamivudine Isentress Ttymp 4 5 6 7 8 2 (21) 3 Length of hospital stay (days) *L-AMB - liposomal amphotericin b
However… ...the patient still had fever... …gradually develops dyspnea along with dry cough… WHAT TO DO NEXT? ESR 96, CRP 56,8 WBC 2,7 (ne 78, ly 7, mo 5, eo 9, pl 1)%, RBC 3,89, HGB 99, HCT 0,294, MCV 75,4, PLT 151 BUN 7,1, SCR 142, Na 140, K 3,6, Cl 103 AST 131, ALT 132, GGT 72, LDH 440, ALP 115 Blood culture: sterile. Urine culture: sterile.
Bilateral diffuse interstitial infiltrates (nodular and linear) Enlarged hilar shadows Chest radiograph, 13th June 2017
Chest CT scan, 14th June 2017 Interstitial lesions that expend from lung apex to bases (spared) Ground-glass opacification
Chest CT scan, 14th June 2017 shows interlobularreticulation and ground-glass opacities
Chest CT scan, 14th June 2017 ground-glass opacification with tree-in-bud pattern
BRONCHOSCOPY • macroscopic findings: moderately expressed bronchial mucosal draft. NAD. • cytological exam: dominantly mononuclear leukocytes with few erythrocytes and rarely a cylindrical epithelial cell. Morphologic shapes which correspond to P. jiroveciare not present. • PCR P. jiroveci–POSITIVE • Mycological – culture and microscopic preparation negative. • Bacteriologically –sterile. • BK – smear negative, culture negative. • PCR CMV 29 020 copies/mL.
26. (24.) 3.-7. (1.-5.) 19. (17.) 12. (10.) DISCHARGE Course of stay L-AMB L-AMB L-AMB L-AMB DH* PROPHYLAXIS (MAC) TRIMETHOPRIM/SULFAMETHOXAZOLE L-Amb4 mg/kg from the day 1 to day 5, and then individual doses on day 10, 17, 24, 31 and 38 *DH – daily hospital
Chest radiograph 3rd July 2017 Regressive dynamics of interstitial lesions
Leishmaniasis • Leishmania spp., family Trypanosomatidae • zoonosis • reservoir – depends on species (dogs, wild mammals, rodents; humans) • vector –order Diptera(so-called Old World – genus Phlebotomus; so-called New World - genus Lutzomyia) • anthroponosis(L. donovani, L. tropica)
Leishmania spp. • family Trypanosomatidae • genus Leishmania • flagellumandkinetoplast (extranuclearDNA within a large mitochondria) • unicellular, obligate intracellular parasite • promastigote form – in biological vector • amastigote form – in mammals • 20 species are pathogen for humans (differentiation is possible with molecular methods, morphological differentiation is not possible)
Leishmaniasis • Leishmaniaspp. • endemic in 98 countries (South America, Africa, South Europe, Asia) • Outside endemic areas – travelers´ diseases • 2 million people • Symptomatic infection– children and HIV positive • Different clinical syndromes
Visceral leishmaniasis (kala-azar, Dum-Dum fever, black fever) Leishmaniadonovani(India, Eastern Africa) Leishmaniachagasi(Central and South America) Leishmaniainfantum(Mediterranean, Middle East, Central Asia and China) 90% cases in three regions: • Indian subcontinent • Eastern Africa • South America (periurban areas in northeast Brazil) • Leishmaniadonovanicomplex: The global incidence of visceral leishmaniasis decreased substantially in the past decade: from between 200 000 and 400 000 new cases in 2012 to between 50 000 and 90 000 in 2017. Prof Davorka Lukas MD, PhD Travel Medicine Conference, Constanca 2018
Croatia • zoophilic Leishmania (L. infantum) • Middle and South Dalmatia • VL – annually five cases • CL - rare • Reservoir– dogs (viscerocutaneous syndrome) • Vector - sandflies
Visceral leishmaniasis (kala-azar, Dum-Dum fever, black fever) • the most severe form of leishmaniasis • symptoms and signs • INCUBATION: 2 – 6 months (10 days to two years or even longer – asymptomatic symptomatic)
HIV+ • Opportunistic infection – people that live/travel to endemic areas • CD4 count <200/𝛍L or during IRIS • Recent infection or reactivation of an asymptomatic infection • Clinical presentation: atypical(bone marrow, lymph nodes, spleen, liver + skin, lungs and gastrointestinal tract) • “Visceralization phenomenon” with species that cause cutaneous forms in immunocompetent hosts
DIAGNOSIS • Clinical presentation and social history • 1. GOLD STANDARD - MICROSCOPY: visualization of the characteristic amastigote in Giemsa-stained smears High specificity, variable sensitivity
DIAGNOSIS • 2. CULTURE • higher sensitivity • Novy-MacNeal-Nicolle (NNN medium) • 24-26˚C, 48-72 h • typization and antimicrobial sensitivity testing 3. PCR • Leishmaniatypization • endemic parts – not an evidence of active infection (detects contact with the parasite– low specificity) • qRT-PCR – differentiates latent from active infection, keeps track of disease progression during treatment (important for HIV+ patients) 4. SEROLOGIC TESTING • diagnostic marker, questionable immunological role