Download
1 / 44
440 likes | 655 Views
Clinical Case 2. 12-year-old boy was admitted to the hospital because of fever, chills, sweats, productive cough, nausea, and vomiting. recurrent pneumonias since the age of 5 years. physical exam: febrile, tachycardic, and tachypneic; diffuse rhonchi in both lungs.

E N D
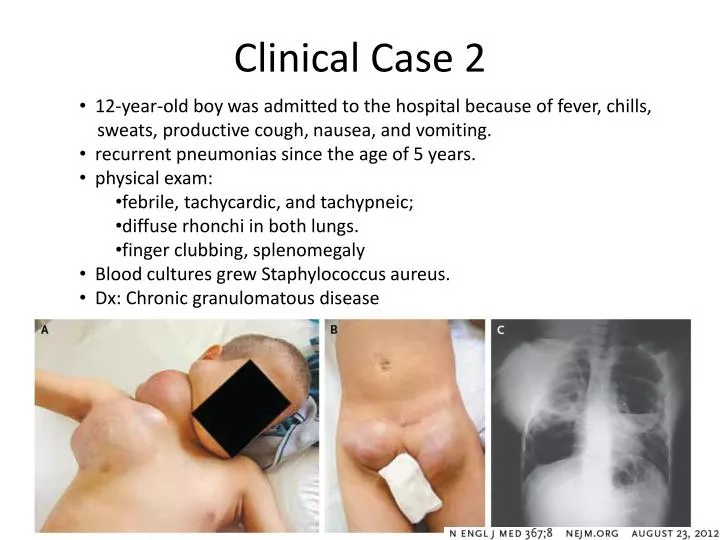
Clinical Case 2 • 12-year-old boy was admitted to the hospital because of fever, chills, • sweats, productive cough, nausea, and vomiting. • recurrent pneumonias since the age of 5 years. • physical exam: • febrile, tachycardic, and tachypneic; • diffuse rhonchi in both lungs. • finger clubbing, splenomegaly • Blood cultures grew Staphylococcus aureus. • Dx: Chronic granulomatous disease
Clinical Manifestations • Disease from S. aureus occurs in one of several ways • toxin formation • localized infection (pyogenic disease) • systemic infection (disseminated infection)
Clinical Manifestations • Staph food poisoning • occurs through ingestion of a preformed enterotoxin (usually staph enterotoxin A or B) in contaminated food • meats, potato salad, custards, ice cream - partially cooked or come to room temperature and then refrigerated • usually the food appears normal • abrupt onset of salivation, N/V, abdominal pain, diarrhea occurring 2 - 6 hours after ingestion • usually occurs in community outbreaks • self-limited: resolves in a few hours
Clinical Manifestations • Toxic shock syndrome • associated with toxigenic staph strains producing TSST-1 • TSST-1: related to the enterotoxins and is a superantigen • patients are colonized with the staph strain and under certain conditions (low oxygen tension, low magnesium concentration, etc), toxin production begins
Clinical Manifestations • Toxic shock syndrome - 2 scenarios clinical picture looks the same • Non-menstrual • usually occurs 48 hours after a surgical procedure • patient looks septic but wound looks good • Menstrual • young women age 15-25 using tampons during menses
Clinical Manifestations • TSS - clinical picture • abrupt onset of myalgias, fever, vomiting, diarrhea • confusion without focal neurologic deficits • severe hypotension, renal insufficiency, shock liver • rash with desquamation of palms and soles within a week - often conjunctival injection
Clinical Manifestations • TSS - Treatment • remove source of the staph (removes toxin production) abscesses, fluid collections, tampons • supportive measures, immunoglobulins, antibiotics • 3% mortality currently - long term neurologic sequelae not uncommon
Clinical Manifestations • Pyogenic disease • Numerous types - clinical name used depends on location and size of the S. aureus infection • Examples: • folliculitis • furuncles/carbuncles - • deep seated inflammatory mass that evolves from folliculitis (zits) - a carbuncle is a coalescence of furuncles • hidradenitis suppurativa • chronic infections of axilla, pubic area associated with apocrine sweat glands
Carbuncle Furuncle
Clinical Manifestations • Pyogenic Diseases con’t • impetigo • Superficial infection of the skin • begins as a vesicular lesion, then changes to a crusty erosion • cellulitis • Infection of the dermal, subcutaneous tissues associated with dolor, rubor, calor, tumor • lymphangitis • Dissemination of infection through lymphatics - can be a complication of pyogenic infection
Clinical Manifestations • SSSS (Staph Scalded Skin Syndrome) • Ritter von Ritterschein disease (in newborns) • Toxins act on the dermis • Generalized • Staph secretes a toxin systemically (usually can’t recover staph from the involved site) • Nikolsky’s sign: detachment of the skin by rubbing • Localized • Bullous impetigo • Blistering around an infected area • Treatment is antistaph agents/local wound care
SSSS vs TEN • TEN (Toxic Epidermal Necrolysis) • Cleavage within the dermis or dermoepidermal junction • epidermal involvement • High fatality rate • Can be difficult to distinguish from SSSS • May need biopsy • Treatment with steroids (?)
Clinical Manifestations • Disseminated infection • “Staph goes where the blood goes” • bacteremia/septicemia usually starts as a local infection and overcomes host defenses • manifestations include endocarditis, vasculitis, pericarditis, pneumonia, osteomyelitis, brain abscess
Treatment • Remove foreign bodies if possible • Drain pus if possible • Duration of therapy depends on the type of infection • bone, foreign body, heart require at least 4 weeks of antibiotics
Treatment • Antibiotic Therapy • guided by local susceptibility data • MSSA- methicillin sensitive S. aureus • good drug choices are B-lactams • Hospital Acquired MRSA (HA-MRSA) • Most frequently due to altered penicillin binding proteins (PBP2a)- mecA gene • resistant to more drugs than CA-MRSA • vancomycin best choice
Treatment • Community acquired-MRSA (CA-MRSA) • doxycycline, trim-sulfa, linezolid, vancomycin good initial choices if CA-MRSA suspected • rifampin resistance occurs rapidly and combination therapy is useful • VISA/VRSA • MRSA that is Vancomycin Resistant • vancomycin intermediate-susceptible MRSA • vancomycin resistant MRSA • consider linezolid or Synercid or daptomycin
Antibiotic Susceptibility Testing Mueller-Hinton Agar Disk Diffusion Vitek 2.0 CA-MRSA
Coagulase Negative Staphylococci • Coagulase Negative staph • 15 species are indigenous to man • 4 are clinically important • S. epidermidis (S. epidermidis) • S. hemolyticus • S. saphrophyticus • S. lugdunensis (infrequent, but severe) • Others: S. capitis, S. caprae, S. warneri, S. auricularis, S. intermedius, S. simulans, S. cohnii, S. chormogenes
S. epidermidis • normal resident bacteria on skin, mucous membranes (S.epi - 65% - 90%) • type, location, and amount of S.epi on skin can be altered by many factors • eg. - antibiotic use, S. aureus colonization • Contains numerous plasmids coding for antibiotic resistance and can easily transfer them within or between species, genus
S. epidermidis • usually highly antibiotic resistant • >80% methicillin resistant • >50% are resistant to: erythromycin, clindamycin, Chloramphenicol, and tetracyclines • Sensitive to: vancomycin, rifampin, and ciprofloxacin • Nearly all infections are nosocomial (hospital acquired)
S. epidermidis S. epidermidis • Coagulase negative • Catalase positive • Growth on blood agar: • Non-hemolytic (gamma hemolysis) • Whitish creamy color • Grows readily (16 hours) S. aureus
S. epidermidis • no known pathogenic exoproteins or toxins • mainly causes infection on “hardware” and is introduced onto foreign body during procedure from hospital environment, hands of personnel • eg - IVs, dacron grafts, CSF shunts, pacemaker wires, artificial valves and joints, implants (breast, eye)
S. epidermidis • Exopolysaccharide layer produced by the organism (biofilm) is the major reason it causes infection on hardware • Biofilm protects S. epidermidis from host defenses such as opsonization and decreases penetration of antibiotics • some surface antigens produced by S. epidermidis may promote its adherence
CoNS Pathogenesis Von Eiff, et al. Lancet Infect Dis 2002;2:677-85
before inoculation 30 minutes 24 hours 12 hours silicone ventricular catheter (Cordis®)
Clinical Manifestations • DO NOT take blood cultures from Lines! • Intravenous Catheter Infections • S. epidermidis- most common associated organism • Can lead to bacteremia and can also be associated with significant morbidity/mortality (“line sepsis”) • Infection can occur at the insertion site or the tip • Remove catheter + Vancomycin
Clinical Manifestations • Bacteremia • S. epidermidis often recovered from blood cultures • most common blood contaminate and rarely causes native valve endocarditis • most common cause of “line sepsis” • major cause of sternal osteomyelitis after cardiothoracic surgery • common cause of prosthetic joint infection
Clinical Manifestations • Infective Endocarditis (IE) • Native valve IE • 5% of all cases are due to S. epidermidis • occurs with seeding of damaged valves, endocardium when S. epidermidis crosses skin barrier • Prosthetic valve IE • 40% of all cases are due to S. epidermidis • if it develops in the first months after valve replacement, seeding probably occurred during surgery
Clinical Manifestations • IE (continued) • Diagnosis • Multiple sets of positive blood cultures • echocardiography • high level of clinical suspicion • Treatment • Vancomycin + gent + rifampin • Removal & replacement of valve
Clinical Manifestations • S. epidermidis endophthalmitis: • Mostcommon cause after cataract surgery/lens implantation • Also occurs in intravenous drug abusers (IVDA) • Dx - clinical exam • Tx - vitrectomy or enucleation with IV vancomycin +intravitreal antibiotics
Clinical Manifestations • Urinary Tract Infections • S. epidermidis usually causes UTIs in elderly, hospitalized patients with catheters in place • Very different than clinical setting of UTIs with S. saprophyticus
S. hemolyticus • (2nd most common cause of CoNS infections) • normal resident bacteria on skin, mucous membranes • Infections: similar to S. epidermidis- • Line infections, endocarditis, septicemia • Others: UTI, Wound, bone, and joint • Lab: similar to S. epidermidis: catalase positive coagulase negative, non-hemolytic on blood agar
S. saprophyticus • Catalase positive • Coagulase negative • Non-hemolytic on blood agar • Novobiocin resistant • True urinary pathogen (rarely a contaminant) • UTI clinical presentation similar to that of infection with GNRs such as E. coli: frequency, urgency, dysuria: pyuria on UA
S. saprophyticus • Infection occurs in healthy young women in an outpatient setting • 70% report sex within 24 hours preceding symptoms • 2nd most common pathogen (after E. coli) in young women • can cause symptoms, pyuria, with <105cfu/ml • may be cause of acute urethral syndrome • Tx - quinolones, Bactrim • may recur in 10% of patients
S. lugdunensis • Infrequent, but important cause of infections • Very aggressive endocarditis with frequent valve replacement, congestive heart failure, and high mortality rate • Bacteremia, arthritis, UTI, central line infections, wound infections • Key lab features: • Beta hemolytic on blood agar • Coagulase negative • pyrrolidonyl-α-naphthylamide hydrolysis (PYR) positive • Detects L-pyrrolidonyl arylamidase • Paper disk impregnated with reagent • (most staph are negative): good rapid screening test • Rapid ornithine decarboxylase positive (all other staphylococci are negative) PYR negative PYR positive
Definitive ID to SpeciesBiochemical Reactions Automated Vitek 2.0 Manual Methods Remel Staph RapID BioMerieux API Staph
Definitive ID to Species 16S rRNA gene sequencing Search Sequence Database of Organisms