Download
1 / 21
260 likes | 595 Views
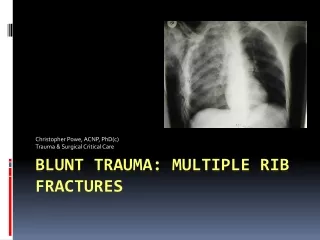
RIB FRACTURES AND THE SERRATUS PLANE BLOCK. Matthew Carr MD PGY-3 Brookdale Emergency Medicine. RIB FRACTURES. RIB FRACTURES. The most common injuries resulting from blunt chest trauma (25%) Usually seen on x-ray But we can also use ultrasound!. ULTRASOUND FOR RIB FRACTURES. Sensitivity

E N D
RIB FRACTURES AND THE SERRATUS PLANE BLOCK Matthew Carr MD PGY-3 Brookdale Emergency Medicine
RIB FRACTURES • The most common injuries resulting from blunt chest trauma (25%) • Usually seen on x-ray • But we can also use ultrasound!
ULTRASOUND FOR RIB FRACTURES • Sensitivity • Ultrasound 80-78% • Plain radiography 23-12% • Clinical acumen 26% • Why does it matter? • Gauge severity of traumatic mechanism • Disposition • Analgesic requirements • Further studies (CT) ACEP guidelines: https://www.acep.org/sonoguide/msk_ribs.html
20 patients with minor blunt chest trauma • X-rays reviewed by 2 radiologists • Ultrasound performed by 1 radiologist • Patients all had negative radiographs • Fractures of the rib, costochondral junction, and costal cartilage were denoted by a clear disruption of the anterior echogenic margin • 26 fractures were found in 18 of the 20 patients • Bottom line: US reveals more fractures
61 patients with suspected rib fractures • US vs. 2 view X-ray • US found 58 rib fractures in 33 patients • X-ray found 32 rib fractures in 20 patients • Also showed that US takes less time than radiology studies • The average duration of USG was (12 ± 3) min (range 7-17 min), whereas the duration of radiography was (27 ± 6) min (range 15-37 min) • US = better and faster than X-ray
METHOD • Linear transducer • Use a lot of gel to minimize pain to the patient • Look in the area of maximum tenderness • Slide along length of rib, can look in both axes • Disruption of anterior cortex • Hematoma • Bending with compression
Rib With compression https://radiopaedia.org/cases/buckle-rib-fracture-on-ultrasound
PEARLS AND PITFALLS • Remember the angle of the ribs necessitates angling of the probe. • Keep the probe perpendicular to the rib surface. • Use a copious gel to enable minimal pressure on a painful area. • Look for multiple fractures when one is found. • Some fractures will show a hematoma around the fracture area ACEP guidelines: https://www.acep.org/sonoguide/msk_ribs.html
Compared injection superficial vs. deep to serratus anterior muscle • Gadolinium and MRI to view spread • Wide spread for superficial or deep injection, more to posterior area when injected superficially • Mean duration of paresthesia: • 752 min for intercostal nerves, 778 for motor nerves after superficial injection • 386 min for intercostal nerves, 502 for motor nerves after deep injection
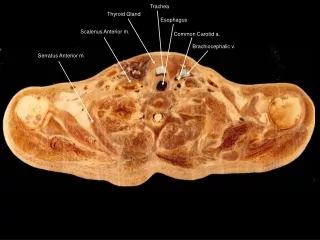
PROCEDURE • Place patient on monitor and pulse ox • Be aware of local anesthetic toxicity symptoms • Position • Lateral decubitus • Supine if lateral decub not possible • Linear probe at 5th intercostal • Transverse plane • Marker facing nipple • Mid-axillary line
PROCEDURE • Clean, prep • Insert needle, in plane approach • Inject 1-2 ml, confirm by seeing fascial plane separate • Inject 2-3 ml at a time, up to 30 ml total • 0.25% bupivicaine
BENEFITS OF THE BLOCK • Adequate analgesia • Decrease the use of opioids • Altered sensorium, decrease in respiratory drive • Maintain pulmonary function, compliance with IS • Prevent pneumonia
RISK FACTORS FOR MORTALITY IN BLUNT CHEST TRAUMA • Systematic review and meta-analysis evaluated risk factors that contributed to mortality in blunt chest trauma patients • Advanced age doubles your risk of death. • Age > 64 had an OR for death of 1.98 (1.86-2.11, 95% CI) • Three or more rib fractures doubles your risk of death • OR of 2.02 (1.89-2.15, 95% CI) • Pre-existing cardiopulmonary disease (CHF) doubles risk of death • OR of 2.43 (1.03-5.72, 95% CI) • Development ofpneumonia has a huge impact on mortality • OR 5.24 (3.51-7.82, 95% CI) Battle CE, Hutchings H, Evans PA. Risk factors that predict mortality in patients with blunt chest wall trauma: a systematic review and meta-analysis. Injury. 2012 Jan;43(1):8-17. doi: 10.1016/j.injury.2011.01.004. Epub 2011 Jan 22.
REFERENCES • Turk F, Kurt AB, Saglam S. Evaluation by ultrasound of traumatic rib fractures missed by radiography. Emerg Radiol. 2010 Nov;17(6):473-7. doi: 10.1007/s10140-010-0892-9. Epub 2010 Jul 23. • Elham Pishbin a, Koorosh Ahmadi b, Molood Foogardi c, Maryam Salehi d, Farrokh Seilanian Toosi e, Vafa Rahimi-Movaghar. Comparison of ultrasonography and radiography in diagnosis of rib fractures. Chinese Journal of Traumatology 20 (2017) 226-228. • ACEP guidelines: https://www.acep.org/sonoguide/msk_ribs.html • R. Blanco, T. Parras,J. G. McDonnell, A. Prats-Galino. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia 2013, 68, 1107–1113. • Nagdev A, Mantuani D, Durant E, Herring A. The ultrasound-guided serratus anterior plane block. ACEP Now. 2017;36(3):12-13. • Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma. 2003;54(3):478-485. • Battle CE, Hutchings H, Evans PA. Risk factors that predict mortality in patients with blunt chest wall trauma: a systematic review and meta-analysis. Injury. 2012 Jan;43(1):8-17. doi: 10.1016/j.injury.2011.01.004. Epub 2011 Jan 22.