Download
1 / 107
1.09k likes | 1.18k Views
ACUTE LEUKEMIA. Definition. PB and/or BM blasts > 20 % of nucleated cell (NC) count. Acute lymphobl a stic leukemia (ALL). Clonal proliferation and accumulation of blast cells in blood, bone marrow and other organs Disorder originates in single B or T lymphocyte progenitor

E N D
ACUTE LEUKEMIA Definition PB and/or BM blasts > 20 % of nucleated cell (NC) count
Acute lymphoblastic leukemia (ALL) Clonal proliferation and accumulation of blast cells in blood, bone marrow and other organs Disorder originates in single B or T lymphocyte progenitor Heterogenous disease with different biological subtypes Incidence in adults : 20% of acute leukemias Etiology - unknown
clinical features 1. Bleeding 2. Fever/infection 3. Bone/joint pain 4. Hepatomegaly 5. Splenomegaly 6. Lymphadenopathy 7. CNS involvement
Patients with very high WBC counts (> 100,000/mm3) are at higher risk for tumor lysis syndrome and leukostasis, both of which are considered oncologic emergencies and require prompt recognition and management. Tumor lysis syndrome can be due to spontaneous or treatment-mediated cell destruction and is characterized by hyperuricemia, renal failure, acidosis, hypocalcemia, and hyperphosphatemia.[Jabbour 2005b
Manifestations of leukostasis include dyspnea, chest pain, headache, altered mental status, cranial nerve palsies, and/or priapism.
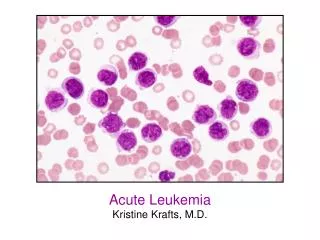
laboratory findings 1. Blood examination - anemia, - thrombocytopenia, - variable leukocyte count, usually increased, - blood morphology: presence of blast cells 2. Bone marrow morphology - presence of blast cells, - suppression of normal hematopoiesis
Laboratory findings 3. Cytochemical stains 4. Immunophenotyping 5. Cytogenetics 6. Molecular studies
ACUTE LEUKEMIA Cytochemistry
Acute leukemia Mixed lineage Vs biphenotypic • Mixed lineage leukemia: • Two different blast populations • Biphenotypic leukemia: • The same blast population bothmyeloid and lymphatic markers AML ALL
EGIL* scoring system for biphenotypic leukemia *European Group for the Immunological characterization of Leukemia To diagnose biphenotypic leukemia, the score should be at least: 2 in the myeloid lineage + 2 in the lymphatic lineage
Acute leukemia ALL with myeloid coexpression Myeloid coexpression= at least20 %of blasts + ve for at least one markerof: CD13,CD33,CD65s.
AL: Immunophenotyping ALL B-ALL (incidence = 76%)
AL: Immunophenotyping ALL T-ALL (incidence =24%)
Acute leukemia WHO Classification of ALL (1999) (1) Precursor B-cell ALL (pro-B, C-ALL, pre-B): (2) Burkitt–cell (mature B-cell) ALL: (3) Precursor T-cell ALL: (4) Mature T-cell ALL:
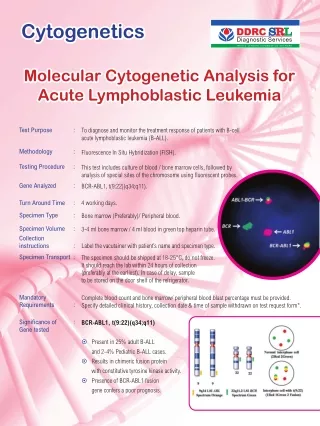
Cytogenetic classification of ALL Bad Prognosis Good Prognosis • Ph-chromosomet(9;22) • *30% of adult ALL • *3% of pediatric ALL • Hypoploidy • (DNA index < 1.12) • t(4;11) • t(12;21) • (Tel/AML1) • *30% of pediatric ALL • Hyperploidy • (DNA index =1.12-1.6)
Algorithm for diagnosis of AL Clinically suspected + blasts in PB Morphology + cytochemistry of PB + BM AML Lymphoblastic lymphoma < 20% blasts in BM < 20% blasts in BM Burkitt lymphoma ALL (L1, L2) ALL (L3) Immunophenotyping B-lineage T-lineage Pro-B C-ALL Pre-B Mature B Early Thymic Mature Cytogenetics / Molecular genetics t (4;11) ALL1/AF4 t (9;22) BCR/ABL
Acute Lymphoblastic Leukemia Outcome • High remission rates possible in adults and children • Leukemia-free survival in children 2-10 years of age: 80% Most adults experience relapse Pui CH, et al. N Engl J Med. 2006;354:166-178.
ALL: Typical Treatment • Induction, consolidation, maintenance phases • CNS prophylaxis with IT-MTX CNS Prophylaxis (IT-MTX) Induction Consolidation Maintenance Over a period of months 2-3 years Free Template from www.brainybetty.com
ALL therapy is one of the most complex types of anticancer programs. Multiple drugs are combined into regimen-specific sequences of various doses and durations. • The backbone of ALL induction regimens is a combination of vincristine,corticosteroids, and anthracyclines. This combination achieves complete remission rates of 72% to 92% with a median remission duration of approximately 18 months
Adult ALL: Large Clinical Trials Free Template from www.brainybetty.com
Prognostic factors in adult ALL (1) At diagnosis Free Template from www.brainybetty.com
Prognostic factors in adult ALL (2) Response to treatment Free Template from www.brainybetty.com
Risk-adapted treatment of ALL Free Template from www.brainybetty.com
Risk-adapted treatment procedure for adult ALL (other than mature B-ALL) Induction (phase I & II) CR Standard risk High risk Consolidation (phase I &II) Donor No donor MRD<10-4 MRD >10-4 HAM Donor No donor Allo BMT Auto BMT End of therapy Allo BMT Maintenance X 2-3 yrs Free Template from www.brainybetty.com
2 Treatment of standard-risk group Free Template from www.brainybetty.com
Treatment of standard-risk group Induction (phase I & II) CR Consolidation (phase I &II) MRD>10-4 MRD<10-4 Donor No donor End of therapy Allo BMT Maintenance X 2-3 yrs Free Template from www.brainybetty.com
Induction treatment of standard-risk group L-Asparaginase 5000U/ m2 30 min inf on saline MTX 15 mg ITH inj 24 Gy DNR 45 mg/m2 VCR 2 mg I.v. VCR/Pred Pred 60 mg / m2 P.O. D1-28 Days 1 7 1 8 15 22 28 Prephase Induction treatment Phase I Free Template from www.brainybetty.com
Details of induction treatment of standard-risk group Prephase If TLC >25000 and/or marked organomegaly • VCR : 2 mg I.V. …………………….… D1 • Pred: 60 mg / m2 P.O. ……………….. D1-7 Free Template from www.brainybetty.com
Details of induction treatment of standard-risk group Phase I induction • VCR: 2 mg I.V. ………………..... D1, 8, 15, 22 • DNR: 45 mg/m2 (30 min. inf.) ..... D1, 8, 15, 22 • L-Asp: 5000 U/m2 ………………. D15–28 • Prednisone: 60 mg /m2 P.O. ...... D1-28 followed by dose reduction in 3 phases of 3 days each: 1/2 1/4 1/8 of the dose then stop. • MTX: 15 mg intrathecal …..……. D1 Free Template from www.brainybetty.com
L-asparaginase in ALL • Used only in ALL • Enzyme that depletes serum L-asparagine • Activity related to serum L-asparagine depletion • No myelosuppression • No late effects • Unique adverse effects Free Template from www.brainybetty.com
L-asparaginase: Toxicity • Hypersensitivity • Neutralizing antibodies • Liver dysfunction • Liver enzymes, bilirubin, low albumin • Hemostasis • Bleeding: low clotting factors • Clotting: low antithrombin III, protein S • Pancreatitis, diabetes mellitus, CNS effects (lethargy, somnolence) Free Template from www.brainybetty.com
There are three formulations of asparaginase available: Asparaginase (L-asparaginase isolated from E.coli ) Erwinia asparaginase (L-asparaginase isolated from Erwinia chrysanthemi, previously called Erwinia carotova6)7 Pegaspargase (L-asparaginase isolated from E.coli and attached to polyethylene glycol) Erwinia asparaginase is serologically and biochemically distinct from asparaginase, although the antineoplastic activity and toxicity is similar. Pegaspargase has a longer half-life and decreased toxicity.
Details of induction treatment of standard-risk group L-Asparginase • Give Erwina-Asp if possible (less adverse reactions) • Check Fibrinogen before giving L-Asp. : • If < 100 mg/dl give FFP 15 ml/kg or 2 gm fibrinogen for correction but continue therapy. • If < 50 mg /dl or prothrombin conc. falls to < 30% stop L-Asp and substitute as above. • Check blood sugar & amylase during L-asp. treatment (3 times / week) and correct hyperglycemia. • The half-life of fibrinogen is 96 hrs. Daunorubicin • DNR dose of day 15 may be omitted if the counts are very low (with no blasts in BM) Free Template from www.brainybetty.com
Details of induction treatment of standard-risk group Cranial prophylaxis • All standard-risk patients receive 24 Gy cranial irradiation • During cranial irradiation, MTX 15 mg intrathecal is given as 4 doses ( twice / week) Free Template from www.brainybetty.com
Although central nervous system (CNS) disease is uncommon at diagnosis (< 10%) in patients withacute lymphoblastic leukemia (ALL), it can increase to as high as 50% to 75% of patients at 1 year without central nervous system (CNS)–directed therapy.
In the absence of IT therapy, isolated CNS recurrence can account for 10% to 16% of relapses, warranting the inclusion of IT chemotherapy in CNS prophylactic regimens. In a study, the use of IT chemotherapy in combination with the hyper-CVAD regimen (hyperfractionated cyclophosphamide, vincristine, doxorubicin, dexamrthasone alternating with methotrexate and high-dose cytarabine) reduced the incidence of CNS relapse to 4%.[Kantarjian 2000]
Details of induction treatment of standard-risk group Phase II induction To be started when neutrophils rise to >1500 /µL and platelets >100 000 / µL. • Cyclophosphamide: • 650 mg/m2 I.V. short inf. …….… D 1, 14, 28 • ARA-C: • 75 mg/m2 short inf. ……………. D 3, 4 , 5 , 6 • D 9, 10, 11, 12 • D 16, 17, 18, 19 • D 23, 24. 25, 26 Free Template from www.brainybetty.com
Details of induction treatment of standard-risk group Phase II induction • In this phase marked neutropenia usually occurs after the 2nd cycle of ARA-C: • As the patient is in CR it is allowed to stop therapy in between cycles until hematological recovery occurs. • Do not reduce doses or leave out cycles Free Template from www.brainybetty.com
Consolidation treatment of standard-risk group Phase I consolidation Triple ITH injection ADR 25 mg/m2 VCR 2 mg I.V. Pred 60 mg / m2 P.O. D1-28 1 8 15 22 28 Days Free Template from www.brainybetty.com
Consolidation treatment of standard-risk group Phase I consolidation • VCR 2 mg I.V. ……………. D1, 8, 15, 22 • ADR 25 mg/m2 I.V. ………. D1, 8, 15, 22 • Pred 60 mg / m2 P.O. ……. D1-28 (then reduced as previously) • Triple intrathecal …………. D1 • ARA-C 40 mg • MTX 15 mg • Dexamethasone 4 mg Free Template from www.brainybetty.com
Consolidation treatment of standard-risk group Phase II consolidation • Cyclophosphamide: 650 mg/m2 short inf. .... D1 • ARA-C: 75 mg /m2 short infusion …………… D 3, 4, 5, 6 • 9,10,11,12 • 100 mg /m2 …………………………..... D 25, 26, 27, 30 • VP16: 100 mg /m2 short infusion ……........... D 25, 26, 27, 30 • Triple intrathecal ………………………………... D1 • ARA-C 40 mg • MTX 15 mg • Dexamethasone 4 mg Free Template from www.brainybetty.com
Consolidation treatment of standard-risk group Maintenance therapy Duration: 2-3 years (depending on MRD study) • 6-MP: 60 mg/m2 P.O. in the morning before breakfast • MTX: 20 mg /m2 I.V. (obligatory) once weekly. CBC should be checked on a weekly basis. Free Template from www.brainybetty.com
Adult ALL: Maintenance Therapy • Weekly methotrexate + daily 6-mercaptopurine • Duration: 2-3 years • Appropriate for all cases except B-cell and Ph+ ALL • Poor outcome if omitted • No randomized trials in adults Free Template from www.brainybetty.com