Download
1 / 47
610 likes | 2.12k Views
Acute Lymphoblastic Leukemia. I2 黃 柏 瑋. Malignancy remains the major cause of death to disease between the age of 1 and 15 years The precise cause of childhood cancer is unknow Leukemia , Neuroblastoma , Wilms tumor , retinoblastoma and tumor of liver. Introduction.

E N D
Acute Lymphoblastic Leukemia I2 黃 柏 瑋
Malignancy remains the major cause of death to disease between the age of 1 and 15 years • The precise cause of childhood cancer is unknow • Leukemia, Neuroblastoma, Wilms tumor , retinoblastoma and tumor of liver
Introduction • Leukemia– the most common malignancy in childhood. • Acute leukemia– 97% Acute lymphoblastic leukemia– 75% Acute myeloblastic leukemia– 20% • Chronic leukemia– 3% Chronic myelogenous leukemia (Ph positive) Juvenile myelomonocytic leukemia ( JMML)
Introduction to pediatric neoplastic disease and tumor • Leukemia and a more pronounced rise in central nervous system tumor • Boy > girl
Leukemia • The most common childhood cancer ( 1/3 of pediatric malignancies ). • Acute lymphoblastic leukemia (ALL) represents about 75 % (peak incidence at age 4 years). • Acute myeloid leukemia (AML) accounts for about 20 % of leukemia (stable from birth through age 10) • Others : CML
Acute Lymphoblastic Leukemia • Childhood acute lymphoblastic leukemia (also called acute lymphocyticleukemia or ALL). • is a disease in which toomanyunderdeveloped infection-fighting white blood cells, called lymphocytes, are found in a child's blood and bonemarrow.
Acute Lymphoblastic Leukemia • These abnormal cells reproduce very quickly and do not function as healthy white blood cells to help fight infection. • the most common form of leukemia • the most common kind of childhood cancer.
Acute Lymphoblastic Leukemia • In the United States, about 3,000 children each year are found to have ALL • Peak incidence occurs from 3 to 5 years of age.
Acute Lymphoblastic Leukemia • the most common symptoms of leukemia:fever, anemia, bleeding and/or bruising ,persistant weakness or tiredness, achiness in the bones or joints, recurrent infections , difficulty breathing (dyspnea) or swollen lymph nodes.
Clinical manifestations • Protean • Bone marrow failure & Organ infiltration • Common symptoms Fever ( 60%) Malaise ( 50%) Pallor ( 40%)
Etiology • Unknown( usually) • Hereditary Down’s syndrome Leukemia in siblings • Chemicals Chronic benzene exposure Alkylating agents • Ionizing radiation • Predisposing hematological disease ( MPD, AA) • Viruses ( HTLV-1)
Diagnostic criteria • ALL is often difficult to diagnose. • The early signs may be similar to the flu or other common diseases.
Diagnostic criteria • bone marrow aspiration and biopsy • complete blood count (CBC) • additional blood tests • computerized tomography scan • magnetic resonanec imaging (MRI) • x-ray • ultrasound • lymph node biopsy • spinal tap/lumbar puncture
Diagnostic criteria • Peripheralblood: anemia,thrombocytopenia, variable white cell count with or without blasts. • Bonemarrow: hyper-or hypo-cellularity with excess of blasts (blasts>30% of nucleated cells).
Diagnostic criteria • Cytochemistry study and surface marker study confirm the lymphoid origin .
Diagnostic criteria • blood tests to count the number of each of the different kinds of blood cells.. • If the results of the blood tests are not normal, a doctor may do a bone marrow biopsy . • The chance of recovery (prognosis) depends on how the leukemia cells look under a microscope.
V-25Leukemic cells in acutelymphoblasticleukemia characterized by round or convoluted nuclei, high nuclear/cytoplasmic ratio and absence of cytoplasmic graulnes.
Differential diagnosis • AML. • MDS. • Non-Hodgkin‘s lymphoma with bone marrow involvement or with leukemic change. • CLL.
Differential diagnosis • Viral infection with lymphocytosis • CML with acute blastic crisis.
Laboratory examinations • Full blood count • Coagulation screening – esp AML M3. • Biochemical screening • Chest radiography • Bone marrow aspiration • Immunophenotyping • Cytogenetics & molecular studies • Lumbar puncture ( CNS involvement)
Complications • Cerebral hemorrhage, pul. hemorrhage or other vital organ hemorrhage. • Infection(sepsis or septic shock ) , pulmonary edema. • Tumor lysis syndrome.
Complications • Infiltration syndrome(CNS, GI tract or gonads). • Coagulopathy before or after chemotherapy. • Anemia.
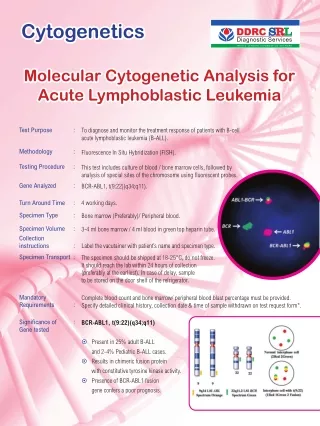
Risk Grouping of TPOG (ALL) • Standard Risk • High Risk– CNS leukemia, cranial nerve palsy, testicular leukemia, pre-B ALL t(1;19) or E2A-PBX1 fusion
Very High Risk • WBC > 100000/mm3 • T – cell • < 1y/o • Lymphoblastic lymphoma with bone marrow lymphoblasts > 25% • t(9;22) or BCR-ABL fusion • t(4;11) or MLL-AF4 fusion • Other MLL gene rearrangement • Hypodiploidy ( chr 44 or less)
Poor Prognosis (I) • Acute lymphoblastic leukemia
Relapse • Bone marrow– the most common site, blast cell increase • CNS– IICP ( vomiting, headache, papilledema, lethargy) Convulsion Behavior disturbance • Testis– painless swelling
Survival rates • 75 % to 80% of children with ALL survive at least 5 years from diagnosis with current treatments that incorporate systemic therapy (e.g., combination chemotherapy) and specific central nervous system (CNS) preventive therapy (i.e., intrathecal chemotherapy with or without cranial irradiation).
Recurrent • The most important extramedullary sites of relapse are the CNS and the testes.
Treatment • Chemotherapy– reach to remission(blast<5%) • CNS prophylaxis Intrathecal C/T Cranial irradiation • Bone marrow transplantation
Management and treatment • Hydration, prevention of hyperuricemia and tumor lysis syndrome. • Antibiotics, may need the 3rd generation of cephalosporin or other strong antibiotics, even antifungal agents.
Management and treatment • Chemotherapy(include remission induction, consolidation & maintenance. • CNS prophylaxis with chemotherapeutic agents(methotrexate 10~15mg, intrathecal injection).
Management and treatment • Blood transfusion(component therapy) • Nutritional support • Bone marrow transplantation • Growth factor
Treatment • The primary treatment for ALL is chemotherapy. • Radiation therapy may be used in certain cases • Bone marrow transplantation is being studied in clinical trials.
Treatment : Chemotherapy • uses drugs to kill cancer cells • drugs may be taken by mouth, or may be put into the body by a needle in a vein or muscle. • All chemotherapy is stopped after two to three years of treatment .
Treatment : Chemotherapy Prednisone: • Used in induction and reinduction therapy and also given as intermittent pulses during continuation therapy. • toxicity : fluid retention, increased appetite, transient diabetes, acne, striae, personality changes, peptic ulcer, immunosuppression, osteoporosis, growth retardation; caution in diabetes, fungal infections, and osteonecrosis
Vincristine: • toxicity : Peripheral neuropathy manifested by constipation, ileus, ptosis, vocal cord paralysis, jaw pain, abdominal pain, loss of deep tendon reflexes; reduce dosage with severe peripheral neuropathy; bone marrow depression; local ulceration with extravasation, SIADH
Asparaginase • local rash, hives, anaphylaxis; bone marrow depression, hyperglycemia, hepatotoxicity, and bleeding may occur. Daunorubicin • Myelosuppression and thrombocytopenia; may cause cardiac arrhythmias immediately following administration and cardiomyopathy after long-term use; nausea, vomiting, stomatitis, and alopecia; extravasation may occur, resulting in severe tissue necrosis; caution with impaired hepatic, renal, or biliary function.
Methotrexate (Folex PFS) • Hematologic, renal, GI, pulmonary, and neurologic systems; discontinue if significant drop in blood counts; aspirin, NSAIDs, or low-dose steroids may be administered concomitantly with MTX (possibility of increased toxicity with NSAIDs, including salicylates, has not been tested)
Radiation Therapy • uses x-rays or other high-energy rays to kill cancer cells and shrink tumors.
Treatmet for VHR Induction:(10 weeks) • Prednisolone,Vincristine,Idarubicin, Asparaginase,cyclophosphamine,cytarabine, 6-MP,TIT. Consolidation:(8 weeks) • 6-MP,MTX,TIT Reinduction:(7 weeks) • Dexamethasone, ,Vincristine,Idarubicin, Asparaginase,cyclophosphamine,cytarabine, 6-MP,TIT.
Bone Marrow Transplantation • Hematopoietic stem cell transplantation is an option for very high-risk cases (e.g., Philadelphia chromosome-positive ALL) or those who develop an early relapse in the bone marrow.
Bone Marrow Transplantation • a newer type of treatment. • high doses of chemotherapy with or without radiation therapy are given to destroy all of the bone marrow in the body. • Healthy marrow is then taken from another person (a donor). • autologous bone marrow transplant, is being studied in clinical trials.
Treatment Induction : 4 weeks • Hyhration. • Allopurinol • Vincristine iv qw & Prednisolone po qd • L- asparaginase • Mediastinum or spine tumor : R/T
Treatment CNS prophylaxis • Intrathecal ingestion : methotrexate • Intrathecal ingestion : methotrexate ,Ara-C, hydrocortisone • High risk:Intrathecal ingestion C/T&R/T