Download

1 / 56
560 likes | 572 Views
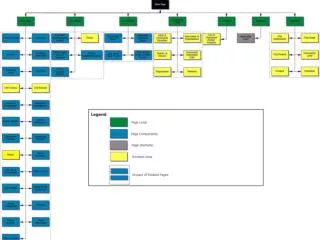
A Blue-Print For The Rural Dental Center Project by Dr. Amit Saini , President of Global Oral Health Foundation Society. Oral health & overall health.

E N D
A Blue-Print For The Rural Dental Center Project by Dr. Amit Saini , President of Global Oral Health Foundation Society
a.Dental diseases are a significant public health burden in India, with dental caries affecting 60 to 65 % and periodontal diseases affecting an estimated 50 to 90 % of the general population, depending on age, with research suggesting that higher rates of dental diseases occur in Rural areas. b.The consequences of widespread poor oral health can be seen on the personal, population, and health systems level, as caries and periodontal disease deteriorate individual health and well being, decrease economic productivity, and act as significant risk factors for other systemic health ailments. ORAL HEALTH a pERSPECTIVE
c.Oral diseases qualify as major public health problems owing to their high prevalence and incidence in all regions of the world. The greatest burden of oral diseases is on disadvantaged and socially marginalized populations. d.Dental diseases in rural India are primarily due to socio-cultural factors, such as inadequate or improper use of fluoride products and a lack of knowledge about oral health and hygiene, and systemic infrastructure deficiencies that prevent proper screening and dental care of oral diseases, especially in rural areas. Oral health a perspective
1.Dental caries are the most common non-communicable disease in the world (Beaglehole, et al., 2009); Periodontal disease and Dental caries are the two dominant disease burdens in oral health. ( By Dr KlingeBeaglehole, Department of Dental Medicine, Division of Periodontology, KarolinskaInstitutet, Stockholm, Sweden.) 2.The need to address these oral health concerns is especially evident in India, because Dental caries affect 60 to 65 percent of the general population (Kaur, et al., 2010). Additionally, Periodontal disease is estimated to occur in 50 to 90 percent of the population in India, depending on age. ( By Dr ArundeepKaur, Professor & HOD, Department of Periodontology, Maulana Azad Institute of Dental Sciences, New Delhi, India. ) 3.The WHO has considered dental caries and periodontal disease to be two of the most important global health burdens because ofthe high worldwide prevalence of both conditions.( Petersen,2003 ).( By Poul Erik Petersen, Chief, Oral Health Programme, WHO, Geneva, Switzerland. ) Dental caries & periodontal
1.Oral cancer is the most common cancer in India amongst men (11.28% of all cancers), fifth most frequently occurring cancer amongst women (4.3% of all cancers) and the third most frequently occurring cancer in India amongst both men and women.( Globcan study ) 2.Oral cancer is a major problem in the Indian subcontinent where it ranks among the top three types of cancer. 3.Oral cancer is of significant public health importance to India. Firstly, it is diagnosed at later stages which result in low treatment outcomes and considerable costs to the patients who typically cannot afford this type of treatment. Oral cancer
4.Secondly, rural areas in middle- and low-income countries also have inadequate access to trained providers and limited health services. As a result, delay has also been largely associated with advanced stages of oral cancer. 5.Earlier detection of oral cancer offers the best chance for long term survival and has the potential to improve treatment outcomes and make healthcare affordable. 6.Thirdly, oral cancer affects those from the lower socioeconomic groups, that is, people from the lower socioeconomic strata of society due to a higher exposure to risk factors such as the use of tobacco. Oral cancers contd:
1.At present the prevention and treatment of oral diseases is virtually unavailable to majority of the population. An Oral Health Strategic Plan is needed to improve the oral health of the people. The Oral Health Strategic Plan addresses the following health outcomes: 1.Reduced incidence & prevalence of dental caries(decay) 2.Reduced incidence of oral cancers. 3.Reduced incidence and prevalence of periodontal Diseases.(gum disease) 4.Reduced disability and handicap resulting from oro-facial defects.(cleft lips and cleft palates) 5.Reduced incidence of oral and facial trauma. Objectives
1.The Project aims to start a fully functional Dental Centre in the village and connecting it with 25 to 30 other surrounding villages thereby covering at least a minimum of 25 villages where the BPL families can get quality dental care under the supervision of Dental Doctor and supporting staff at highly subsidized costs to them. Also, the middle class & affluent section of people living in these villages can access dental care at a reasonable cost to them thereby cross subsiding the Dental treatment expenses towards the BPL families. 2.Dental Awareness Camps to be held twice a month by the NGO in the surrounding villages with the assistance of the ASHA Workers so as to make the people aware of the Oral Health Diseases and also to discuss preventive methods with regards to Oral Health. MISSION
A. I had in this mission, conceptualised and set up the Dental Department at ShriNabhKanwal Raja Sahib Charitable Hospital at Village MazaraNau-Abad in Nawanshahr-Punjab in the year 2007. This Dental Department went on to provide Dental Healthcare Treatment to the people living in the village and also to the surrounding villages at highly subsidised costs. It revolutionized Oral Healthcare among the rural areas in approximately around a belt of 150 Villages. B. Manypatients had come for their First visit to a Dentist such was the neglect about their Oral Health. This translates into the lack of knowledge/awareness about Oral Health and Hygiene among the rural populations. Has the ngo tested the solution?
1.I have seen from close quarters while working as a Consultant and Head In-Charge of the Dental Department with a Charitable Hospital situated in the rural hinterland, the day to day hardships borne by the poor and the marginalized sections of people in receiving quality dental care at the hands of the Dental Professionals. 2.Public Expenditure on Health as percentage of GDP by Government has varied from 1.12% ( 2009-2010) to 1.18% (2016-17 ).Meanwhile, States spending in the same period has risen from 0.7% of their GDP to 0.9% the health ministry claims.This, experts suggest, is a measly amount when compared to the country’s needs. Introduction
3.With government spending on healthcare stagnating over the past decade, the private healthcare industry has boomed. This has meant that people continue to spend high amounts from their pockets as costs of medical care rise over time. 4.That public spending is not meeting people’s health care expenditure needs is evident from out-of-pocket-expenditure data compiled by the World Bank. In the year 2014-’15, 62.42% of health spending was borne by citizens. Ideally, when a country’s public healthcare system is improving, the out-of-pocket-expenditure as a percentage of total health expenditure should come down. In India’s case it only has reduced marginally, from 63.37% in 2010 to 62.4% in 2015. Introduction-1
5. National Health Mission (NHM)one of the main programmes of the Government includes 4 Components. Mission Flexipool covers as many as 29 activities/ Programme/Scheme out of which NOHP is one. NOHP comes under the NHM in the category Flexible Pool for Non-Communicable Diseases, Injury & Trauma. Thus Oral Health has to compete along with the Other Programmes for Funds. 6.The Govt. has decided now that National Oral Health Program (NOHP),would be a part of Health system strengthening under NRHM (also known as Mission Flexible pool). Approvals will be given to the states in NOHP under Health system strengthening under NRHM. The Utilization Certificate(UC)under the pool of system strengthening will cover the utilization of NOHP. Introduction-2
7. The most accessible and Principal healthcare provision facilities for rural India, Primary Health Centers (PHC)do not provide Dental Services and only 20-25% of Community Health Centers, the point of secondary healthcare for rural villages within the Indian Healthcare System, provide Dental Care. 8.In Rural India, the dentist to population ratio is as high as 1 Dentist for every 250,000 residents whereas in Urban India the ratio is I Dentist per 10,000 population. This vast striking imbalance seen of the Dental Professionals not working in the rural areas acts as a major barrier for the rural people to access quality dental care. 9.Another major factor that acts as an Barrier is the high cost of dental treatment. The poor and underprivileged sections of people in the rural areas thus cannot access the Private Dental Clinics in the nearby towns because of the high costs involved. Introduction-3
10.Thus they are left with no option but to avail the services of the Quacks (Unqualified Professionals) because of the low costs .There are about 100,000 Quacks who are providing crude dental care in the rural parts of India. Thus the villagers often end up with serious consequences to their Oral Health at the hands of these Quacks. 11.It has been established that Rural India is experiencing wide-spread challenges in oral health. It can be further said that these challenges exist at every level of the healthcare infrastructure, from a lack of dissemination about preventative oral health education to severely restricted access to curative dental treatments. INTRODUCTION-4
12.Only 15-20% of people living in India are able to get dental services through national schemes. 80-85% of people are spending money from their pocket. Although huge unmet treatment needs exists; striking inequality in delivery system, and absence of an adequate community-oriented prevention system is further aggravating the lack of reach of dental facilities in rural parts of India. 13.Thus this Project plans by the opening of Rural Dental Centres in the villages across India aims to: a.Increase awareness of the importance of Oral Health. b.Improve access to Dental Services in Rural India under the supervision of a qualified dental surgeon and supporting staff. c.Prevention of Oral Cancer. INTRODUCTION-5
It is to this section of society that I would like to target and bring back smiles on their faces. PLEDGE
A.The Project aims to start a fully functional Dental Centre in the village and connecting it with 25 to 30 other surrounding villages thereby covering at least a minimum of 25 villages where the BPL patients can get quality dental care under the supervision of Dental Doctor and supporting staff at highly subsidized costs to them.( HUB & SPOKE Method) B. Also,Dental Awareness Camps to held twice a month by the NGO with the assistance of the ASHA Workers so as to make the people aware of the Oral Health Diseases and also to discuss preventive methods with regards to Oral Health. C.The middle class & the affluent section of people in these villages will get dental treatment at a reasonable cost thus cross subsidizing the Dental Treatment to the BPL Families. The proposed plan-page 1
2.The Various Manufacturers of Dental Equipment's can help in sponsoring a Dental Chair Unit and Dental Equipment's for basic dental procedures. 3. The Dental Chair Unit can be sponsored by Confident, a Leading dental chair manufacturer in India. 4. The toothpaste and other Oral Products can be sponsored by Colgate India as part of their Bright Smiles Bright Future Initiative. 5. Recruitment of a Computer Professional who will digitally record the patients history & Clinics work. 6.Desktop Computer to be sponsored by HP alongwith 3-in-1( Print/Copy/Scan )to be sponsored by Canon India. The proposed Plan—page2
7.The medicines can be sponsored by SUN PHARMA as part of their Corporate Social Responsibility. 8.Recruitment of a Dental Doctor willing to work in the rural hinterland to serve the people. 9.Recruitment of a Dental Assistant to be done from the local population who will help in taking care of dental emergencies after doctor’s duty hours. 10.Construction of a Toilet in the Dental Center by Sulabh International for the patients and the Staff. The Proposed Plan-Page 3
11.The Dental Center will be equipped with Teleconferencing facility so as to interact with Dental Experts via Airtel 4G Broadband Services. 12. The Dental Center will have clean drinking water facility on its premises which can be provided by Tata Swach RO Filters for the patients and the staff. 13. The Dental Center will be equipped with a Generator of 5KVa which can be provided by KirloskarGensets for uninterrupted electricity in the smooth running of the Dental Center. 14. The Dental Center will be equipped with a Camera and DVR to see the working of the Center on daily basis by both the Parties. The Proposed Plan—Page 4
This Project will be transparent and accountable to its various stakeholders by the following proposals: • Stock Registrar on daily basis reporting • Receipt & Payment, Income Expenditure and Balance Sheet to be prepared on a Quarterly basis and provided to the NGO & the Facilatator. • Facilatator and the NGO will share the area reviews and Project screening on periodically basis. • Camera to see the working of the Dental Centre in real time mode to be viewed by both the NGO and the Facilatator. TRANSPARENCY & ACCOUNTABILITY
Monthly Audits to see the working of the Dental Centre with regards to: 1.How many patients treated and their monthly treatment plan. 2.Verify the above claim by meeting selected patients through a random sampling. 3.All Complete Denture Cases to be verified every month by personal physical inspection and taking their photograph with thumb impression/signature for official record. assessing EffectiVeness
a. Because fluoridated toothpaste is a highly effective means of caries control, every effort must be made to develop affordable fluoridated toothpastes for use in developing countries. The use of fluoride toothpastes being a public health measure, it would be in the interest of countries to exempt them from the duties and taxation applied to cosmetics. b. Salt fluoridation as a means of population-wide fluoride supplementation should be considered. This method of salt fluoridation could be easily implemented across the rural hinterland in India as a low economic cost to the Governments especially targeting the rural people in prevention of caries. Way forward
This is the Blue Print to roll out an effective program of rural dental health services across the villages pan India. This program can be effectively rolled out across the length and width of state/country in a phased manner. I have made my presentation and now I await the response of the Stakeholders in this noble endeavor. Way forward
1.The Project was awarded the Karmaveer Chakra, 2012 by International Confederation of NGO’s( iCONGO ) during the REX Conclave held in Delhi in 2012 in association with UN. Website of the Organization: http://www.rexideas.com/ 2. Have spoken lately via Skype to the Delegates of the India Development Coalition of America (IDCA) on the Rural Dental Center Project at their 6th North India Conference held at IIIM, Jaipur on 3rd March 2017. Website of the Org: https://www.idc-america.org/ Awards by the ngo
3.My Nomination for Participation as Innovator/Startup has been selected for RISC 2017 being held in Hyderabad on 23-24 March 2017. The Event is being conducted by National Institute of Rural Development & Panchayati Raj( NIRDPR ). Website of the Org:www.nird.org.in // www.risc2017.com 4. I have also been selected for the South Asia Leaders Program being conducted by Common Purpose India for the Event to be held from 22 - 25 May 2017, Mumbai & 22 - 25 August 2017, Colombo respectively. Website of the Org: www.commonpurpose.org RECOGNITIONS TO THE NGO:
5. Today as on 29 May 2017, I received a mail from MaD ( Make a Difference ) Festival for their Event Participation in Hong Kong. Confirmation Letter of MaD Festival 2017 - International Assembly This is to certify that Mr. AmitSaini is selected as one of the participants of the MaD Festival 2017 - International Assembly in Hong Kong under the Asian Subsidy Scheme which partially financially supports the accommodation and airfare of our participants. Details of the event is provided below: Date: 21 - 23 July, 2017 Venue: KwaiTsing Theatre, Hong Kong Website of the Organisation: http://www.mad.asia/ RECOGNITIONS TO THE NGO:
6.Invitation by DESHPANDE FOUNDATION for their Development Dialogue Conference 2018 to my good self Development Dialogue 2018! Development Dialogue is India's most awaited social entrepreneurship ecosystem conference, hosted by the Deshpande Foundation at Hubballi, Karnataka. You are invited for the 2018 Dialogue scheduled for February 3rd and 4th. Pre-events include a Sandbox immersion field visit on February 2nd and a week-long community-driven conclave from 25th to 29th January. To learn more visitwww.developmentdialogue.org RECOGNITIONS CONTD:
I have been invited by Dr Raman Bedi for the Senior Dental Leadership Programme in the UK in 2018. Mr Bedi has said that I wish to come then the Global Child Dental Fund will waive off 50% of my registration fee of 10,000 US Dollar. It is the best opportunity to learn from the Leaders in Oral Health and get the same replicated back home in India. Though it is an excellent opportunity but the remaining 5000 US Dollars is still too High for myself to attend. It is my earnest appeal to Organisations / Foundations to back me so that I can contribute towards Oral Health in a more meaningful way and contribute towards the Oral Health Sector in India by working with them. 7. Senior dental leadership- 12
I am sharing with you all the Consolidated Statistics of the First 20 Dental Camps conducted by the NGO along with the Results . In this, I was helped by a Technology Partner. The Technology partner is helping the Foundation record, track and manage the patient visits to bring accountability and transparency in the operations. I am sharing the Link with you all with a Brief Write-up of my Observations during these Camps: https://drive.google.com/open?id=0B8-CdGuIFX4-enQzN3lfQl91OTA WORK DONE BY THE NGO TILL DATE:
1. About 50% of the Female Patients were from 20-40 yrs Group. 2. 70% of the Male Patients were from below 40 years. 3. 50% of the patients examined ( male & female both ) had poor Oral Hygiene and were advised Oral Prophylaxis ( professionally cleaning of teeth by a Dentist / Dental Hygienist ) 4. A majority of the Children over 40% under the 20 years Age Group had Carious teeth. This was because of lack of knowledge about Oral Health & Hygiene among Children. The Clinical Findings of the Dental Camps: