Download
1 / 47
470 likes | 589 Views
Project Blue Print CAPTASA Conf. By Gary D. Carr, MD, FAAFP Diplomate ABAM Past President FSPHP. Why Study PHPs. PHPs claim an amazing success rate. Is it true? If it is true, why? Are their implications for society in general? We have high profile detractors

E N D
Project Blue PrintCAPTASA Conf. By Gary D. Carr, MD, FAAFP Diplomate ABAM Past President FSPHP
Why Study PHPs • PHPs claim an amazing success rate. Is it true? • If it is true, why? • Are their implications for society in general? • We have high profile detractors • A sensation-driven News Media does not consider a success story newsworthy
The Investigators • Tom McLellan, PhD • Bob DuPont, MD • Greg Skipper, MD • FSPHP Steering Committee Grant from Robert Wood Johnson Foundation
Study Design • Physicians Only • Questionnaires • Retrospective Study: Phase I & II • Tested by 5 PHPs • F/U Calls • Steering Committee Adjustments.
Phase I • Structure and Function of PHPs • Survey 49 states • 42 (86%) Responded • Physicians entering before 9/01 • Cases taken sequentially
PHP Affiliation • 54% Independent 501c3 Corp • 35% Component of Med. Assoc. • 10% Board Run
Physician Health Issues Addressed • Substance Use Disorders -100% • Psychiatric Illness - 85% • Distressed Behavior - 79% • Physical Illness - 62% • Other - 18%
Professions Served • Physicians Only 36% • Physicians and Others 64% Dentists 51% Veterinarians 33% Podiatrists 23% Pharmacists 21% Others 18%
PHP Referral Sources State PHPs Board 21% Self 26% Colleagues 22% Med Staff 14% Other 17%
Authority • All claim some agreement or memorandum of understanding with their state board 71% formal 29% informal • Legal authority – 76% 59% - specific state laws 20% - peer review laws 21% - other (Contract)
Funding The Avg PHP Funding Sources Boards 50% Participants 16% Medical Assoc. 10% Hospitals 9% Malpractice Carriers 6% Other 10% i.e. The average PHP receives 50% of its funding from the state Board
Other PHP Characteristics • Paid PHP Staff 1 – 19 c average = 5 • Budget - $21,000 – 1.5 million c Avg = $538,000 • Avg no. of New A & D Cases/PHP/Yr Avg 34 / yr (range 0 – 150) • Avg caseload – 138 physicians Range – 9 – 541 Total 5,091 monitored by 37 state PHPs
Drugs of Abuse • 49% - Alcohol • 35% - Opioids • 8% - Stimulants • 5% - Sedatives • 3% - Marijuana • 2% - Other • Alcohol Only – 37% • Drugs Only - 27% • Both - 31%
Co-occurring Psychiatric Illness • 37.4% Average • 40% Median • Range 16% - 65% • Probably skewed. More reasonably 40 – 50 %
Specific PHP Activities/Requirements State PHPs Interventions 100% Evals by Referral 71% Eval by PHP 18% Caduceus Groups 95% Outside Psychotherapy 97% 12 Step Programs 94% Drug Testing 100% Outside TPA 66% In House 34% Approved Eval/TX Centers76% Require Progress reports 95% Worksite Monitors 71%
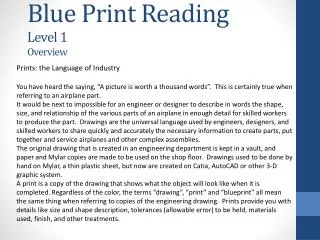
Types of Material Drug Tested* * N = 36 Programs Responding
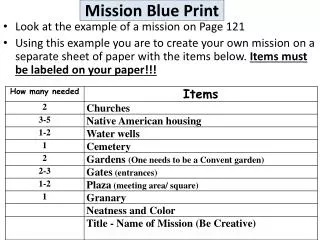
Types of Drug Test Panels Used* * N = 36 Programs Responding
Frequency of Drug Tests • Compared the first and last years of contract • Physicians are tested for drugs an average of 4 times per month in the first year of their contract for a total of about 48 tests in initial year • Range = 12 to 120 tests per physician • By the final year of the contract, the average frequency of testing is about 20 tests per year • Range = 4 to 72 tests per physician • In general, PHPs tend to increase the frequency of testing if there has been a positive test * N = 40 Programs Responding
Randomization of Drug Tests • All PHPs conduct random drug testing • 22 of 39 (56%) test only during the week • 16 of 39 (44%) test randomly including weekends. * N = 39 Programs Responding
EtG Testing • 41% of physicians routinely receive EtG testing • 43% receive it on an as needed basis • Cutoff level used for EtG testing varies from 100 to 500 ng/ml with the average being approximately 250 ng/ml * N = 36 Programs Responding
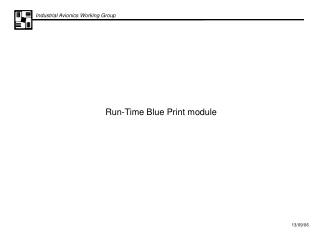
Board Reporting Requirements * N = 35 Programs Responding
Programs Participating • All programs invited • 16 PHPs agreed to participate • Western – 3, Central - 2, SW - 1, SE - 6 and NE – 4 • Chart review instrument developed • < 120 physician chart reviews per program • PHP Staff paid $20 per chart
Inclusion Criteria • Physicians only • Must have signed a contract including DOA testing before 9/1/01 • Chart must be taken sequentially in order proceeding to next previous • 908 chart reviews submitted • 4 excluded – did not meet inclusion criteria • Average 7.2 year Follow-up • 904 total included in study
Prior History with PHP? • 77% - No • 23% - Yes 61% - 1 prior contract 18% - 2 prior contracts 13% - 3 prior contracts 5% - 4 prior contracts 3% - 5 or more
Prior History of Substance Use Disorder Treatment? • Yes – 39% • No - 61% Of the 39% with prior treatment… In Your PHP During prior Treatment? • Yes - 42% • No - 58%
Specialties • Overrepresented • Anesthesiology, Emergency Medicine, Psychiatry, and Family Practice • Underrepresented • Pediatrics, Surgery, Pathology
Use of Medication to Treat Addiction • Only one individual, of the entire 906 physician cohort, was placed on methadone (no other agonist therapy used). • Naltrexone was used in 46 (5%) of individuals as an adjunct to treatment, • 32% were placed on antidepressants.
Relapse (N=904) • Level I Behavior w/out use 15% • Level II Outside of practice 16% • Level III In context of practice 6% • Substance Relapse (Level II/III) in PHPs-22% over an average of 7.2 years monitoring !!!
Relapse • A total of 73,942 drug tests were performed 162 (18%) participants had at least one positive drug test. • 199 participants were reported as having relapsed, (Relapses of 37 (19% of relapses) participants were diagnosed by other means than a positive drug test. • Relapse rate of 22% for participants over the entire monitoring period of 7.2 years (avg). • Same relapse rate (22%) as previous ten year study of Washington State PHP (Domino et al).
Outcomes • 78% - Maintained sobriety over avg 7.2 years • 22% - Relapse (n = 199) 102 (55%) reported to Board • 11% - Report to Board w/out relapse
Outcomes: Relapse and Report to Board • N = 102 physicians relapsed and reported to Board • 66% had action taken 18% - Practice Limitations 18% - Public Probation Agreements 23% - License Suspension 8% - License Revocation 9% - Loss of DEA 18% - Managed by PHP 16% - Non-public probation
Actions Against Physicians Who Did Not Experience Relapse • 40% of Physicians w/out relapse had adverse action 14% - Public Probation 13% - Non-public Probation 7% - Suspension 6% - Practice limitations 2% - Revocation
Most Recent Status of Medical Practice FSPHP • Full Time Practice 74% • Part Time Practice 2% • Licensed. No Practice 5% • Not Licensed 11% • Other 11% (May exceed 100%)
Outcomes of Study Participants (N = 904) FSPHP • Successfully Completed 66% • Continued Monitoring 11% • Appropriate Transfer 8% • Died 2% • Moved. Lost to F/U 5% • D/Ced by PHP 6% • Suicide 1% (May exceed 100%)
Patient Safety? • One (1) Report of Patient Harm – Overprescribing • Consistent with earlier study of 259 physicians monitored over 11 years that failed to document even one case of patient harm. (Domino)
Some Important Findings • 78% Total abstinence x 7.2 yrs • 6% Relapse in context of medical practice • Only 1 report of pt harm (overprescribing) • PHPs are not utilizing medications proven helpful (i.e. Naltrexone, Antabuse, Vivitrol, etc) • More punitive states do not have better outcomes.
Conclusions • PHPs are effective • Addiction is highly treatable • Recovering Doctors can practice safely
Conclusions • Many possible reasons physicians do well: • Wealth, position, family supports • Higher quality care • Most Important: Monitoring with support & contingency plan
Conclusion • Long-term monitoring with support & contingency plan: May be the missing component to improve addiction treatment outcomes! • May be the key for PHPs • May be the key for Drug Courts • May be the key for public at large?
Contact Me Gary D. Carr, MD, FAAFP Diplomate ABAM Medical Director Emeritus PHN Past President FSPHP BRI II Office: Southern Neuro and Spine Institute 1 Lincoln Parkwaqy Suite 303 Hattiesburg, MS 39402 Cell No. 601-297-6777 Email – Docgcarr@aol.com