Download
1 / 13
130 likes | 442 Views
Dr. Laila Al Dokhi Assistant Professor Department of Physiology. Lecture 1 Hypothalamic and pituitary gonadal axis. Objectives. By the end of this lecture, you should be able to: Define hormones Characterize hypothalamic pituitary relationship

E N D
Dr. Laila Al Dokhi Assistant Professor Department of Physiology Lecture 1Hypothalamic and pituitary gonadal axis
Objectives By the end of this lecture, you should be able to: • Define hormones • Characterize hypothalamic pituitary relationship • Name the hypophysiotropic hormones and outline the effects that each has on anterior pituitary function • Name anterior pituitary gonadotropic hormones and outline the effects that each has on the gonads • Describe the negative and positive feedback mechanisms in the hypothalamic-pituitary-gonadal axis and their importance in the control of reproductive function Keywords: hypophysiotropic hormones, gonadotropic hormones, androgens, estrogens
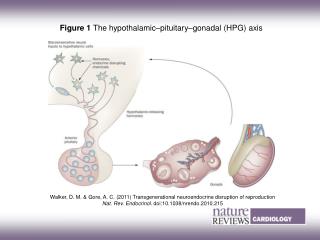
Definition of hormone: Chemical substance (messengers) produced by ductless glands that are transported in the circulation to the target cells where they regulate the metabolic processes. The connection between the hypothalamus and pituitary gland via: • Hypothalamohypophysial tract between the posterior pituitary gland, supraoptic and paraventricular nuclei (neural connection) • Hypothalamic hypophysial portal vessles between the anterior pituitary gland and the hypothalamus The anterior pituitary secretes six hormones: • Adrenocorticotropic hormone (corticotrophin, ACTH) • Thyroid-stimulating hormone (thyrotropin, TSH) • Growth hormone (GH) • Follicle-stimulating hormone (FSH) • Luteinizing hormone (LH) • Prolactin (PRL)
Control of male sexual functions by hormones from the hypothalamus and anterior pituitary gland: GnRH and its effect in increasing the secretion of LH and FSH: GnRH peptide secreted by the arcuate nuclei of the hypothalamus through the hypothalamic-hypophysial portal system to the anterior pituitary gland and stimulates the release of gonadotropins (LH and FSH). GnRH is secrete intermittently for few minutes every 1 to 3 hrs. The secretion of LH by the anterior pituitary is also cyclical flowing the pulsatilerelease of GnRH.
Testosterone regulation of its production by LH: Testosteroneis secreted by leydig cells, in the interstitium of the testis, by LH stimulation from the AP and its release is directly proportional to the amount of LH. Mature leydig cells are found in infants testis few weeks after birth & then disappear until puberty when it appear again. Inhibition of anterior pituitary secretion of LH and FSH by testosterone – negative feedback control of testosterone secretion: Testosterone secreted by the testis in response to LH stimulation and has reciprocal effect of inhibiting the AP secretion of LH. Most of the inhibitory effect result from a direct effect of testosterone in the hypothalamus to decrease secretion of GnRH which causes decrease secretion of both LH & FSH.
Regulation of spermatogenesis by FSH and testosterone: • FSHbinds with specific FSH receptors attached to the sertoli cell in the seminiferous tubules, which causes these cells to grow & secrete spermatogenic substances. Also testosterone & dihydrotestosterone diffuses into the seminiferous tubules from the leydig cells affect the spermatogenesis, so both FSH & testosterone are necessary to initiate spermatogenesis. Negative feedback control of seminiferous tubule activity – role of the hormone inhibin: • When the seminiferous tubules fail to produce sperm secretion of FSH from the AP increases. Conversely, when spermatogenesis proceeds rapidly pituitary secretion of FSH diminishes. This is due to the secretion of inhibin hormone from the sertoli cells which strongly inhibit the AP- FSH and slight inhibitory effect on the hypothalamus to inhibit GnRH secretion.
Regulation of the female monthly rhythm, interplay between the ovarian and hypothalamic-pituitary hormones: • Secretion of AP hormone is controlled by “releasing hormones” formed in the hypothalamus and transported to the AP gland by the hypothalamic-hypophysial portal system. • Intermittent, pulsatilesecretion of GnRH by the hypothalamus stimulates pulsatile release of LH from the AP: GnRH is secreted in pulses lasting 5 to 25 minutes every 1 to 2 hrs. The pulsatile release of GnRH cause intermittent output of LH secretion about every 90 minutes. Hypothalamic centers for release of GnRH: The neural activity that causes pulsatile release of GnRH occurs in the mediobasal hypothalamus, in the arcuate nuclei regulate most of the female sexual activity.
Negative feedback effects of estrogen and progesterone in decreasing both LH and FSH secretion: • Estrogen in small amounts has strong effect to inhibit the production of LH & FSH. This inhibitory effect of estrogen is increased when progesterone is available. This inhibitory effects more on the AP directly & to lesser extent on the hypothalamus to inhibit the secretion of GnRH. Hormone inhibin from the corpus luteum inhibits FSH & LH secretion: • The hormone inhibin secreted by the granulosa cells of the ovarian corpus luteum inhibit the secretion of FSH & to lesser extent LH.
Positive feedback effect of estrogen before ovulation – the pre-ovulatory LH surge: • AP secretes increased amount of LH for 1 to 2 days before ovulation. FSH surge is much smaller in the pre-ovulatory than LH surge. The possible causes of LH secretion could be: • estrogen has special positive feedback effect of stimulating pituitary secretion of LH & to a lesser extent FSH • the granulosa cells of the follicle begin to secrete small increasing amount of progesterone about 1 day before ovulation which stimulate LH secretion
Feedback oscillation of the hypothalamic-pituitary-ovarian system: Postovulatory secretion of the ovarian hormones, and depression of the pituitary gonadotropins: During the postovulatory phase (between ovulation & beginning of menstruation) the corpus luteum secrete large quantities of both progesterone &estrogen & inhibin which all together cause negative feedback effect on AP & hypothalamus to inhibit both FSH & LH secretion. (lowest level 3-4 days before the onset of menstruation)
Follicular growth phase :- • 2 to 3 days before menstruation, corpus luteum regress & secretion of estrogen, progesterone & inhibin decrease. • This decrease remove the negative feedback effect on AP hormones. Therefore a day after menstruation FSH secretion begins to increase (2 folds) while LH secretion is slightly. These hormones causes growth of the follicle. During the first 11 to 12 days of this follicle growth the rate of secretion of FSH & LH decrease slightly because of the negative feedback effect of estrogen on the AP. Pre ovulatory surge of LH & FSH causes ovulation: • About 12 days of the monthly cycle, the high secretion of FSH & LH start to increase due to high level of estrogens causes positive feedback on the anterior pituitary which leads to pre-ovulatory LH surge & FSH surge.