Download
1 / 18
180 likes | 289 Views
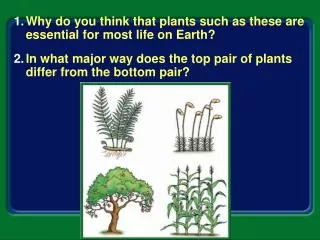
ESSENTIAL LIFE PLAN (by Isobel Allan Mother & Carer). SUSIE ALLAN 2008. WHAT IS AN ESSENTIAL LIFE PLAN?. A WRITTEN DOCUMENT THAT OFFERS A HOLISTIC ACCURATE AND DETAILED ACCOUNT ON THE NEEDS, ABILITIES, DIFFICULTIES AND LIMITATIONS OF SOMEONE WHO HAS COMMUNICATION PROBLEMS

E N D
ESSENTIAL LIFE PLAN(by Isobel Allan Mother & Carer) SUSIE ALLAN 2008
WHAT IS AN ESSENTIAL LIFE PLAN? • A WRITTEN DOCUMENT THAT OFFERS A HOLISTIC ACCURATE AND DETAILED ACCOUNT ON THE NEEDS, ABILITIES, DIFFICULTIES AND LIMITATIONS OF SOMEONE WHO HAS COMMUNICATION PROBLEMS • A ‘LIVING DOCUMENT’ THAT IS CONSTANTLY UPDATED, MIRRORING THE LIFE JOURNEY OF THE PERSON
WHY HAVE AN ESSENTIAL LIFE PLAN? • TO MAINTAIN CONSISTENCY AND AVOID OMISSION IN CARE AND SUPPORT • TO ENSURE ONE CORE DOCUMENT, THAT SURPASSES ALL OTHERS • TO ENSURE THE SAFETY, HEALTH AND WELLBEING OF THE PERSON • TO REDUCE THE WORKLOAD ON CAREGIVERS (STAFF) BY HAVING ONE MAIN POINT OF REFERENCE • TO RESOURCE ALL CAREGIVERS WITH THE SAME INFORMATION AND FACTS AT THE SAME TIME (within a continuum)
WHO SHOULD CONSTRUCT, MAINTAIN AND UPDATE THE PLAN? • THE PERSON WHO LIVES THE LIFE • IF THE ABOVE IS NOT POSSIBLE> THE MOST CONSTANT SOURCE WITHIN THAT PERSONS LIFE (USUALLY THE MAIN CAREGIVER) SHOULD BE RESPONSIBLE
WHO SHOULD OFFER INPUT/ BE CONSULTED/ INVOLVED IN THE PLAN? • THOSE WHO OFFER SPECIFIC INPUT OR SUPPORT, THIS COULD INCLUDE e.g. > The person, Their family, Family GP, Day Centre, Respite Unit, In Home Support Services, Personal Assistant, Social Worker, Learning Disability Nurse, Key worker, Specialised Input (healthcare/physio etc)
HOW IS THE PLAN CONSTRUCTED? • EVERY PERSON HAS> NEEDS ABILITIES DIFFICULTIES LIMITATIONS NEEDS ABILITIES DIFFICULTIES LIMITATIONS
HOLISTIC AND PERSON CENTRED APPROACH IS ESSENTIAL FOR THE LIFE PLAN>
A COMPLETE PERSON> Needs Physical Intellectual Emotional Social Spiritual Difficulties Abilities Limitations
THE CREATION OF THE ESSENTIAL LIFE PLAN> • One main co-ordinator (either the person or the most constant source in that persons life) • Use the *P.I.E.S.S. model as a template, plus include the needs, abilities, difficulties and limitations in each of the *above • Keep the contents> person centred, simple, accurate, relevant, (without jargon), factual, meaningful, real, descriptive, holistic, dated, itemised. Mirror the person & their life • Formulate first draft/future revisions of the essential life plan and send to all relevant ‘key players’ with deadline for feedback
THE CREATION OF THE ESSENTIAL LIFE PLAN> • When relevant and appropriate, seek any additional input (e.g. physiotherapist, GP etc) • Finalised Plan (due to consultation/involvement) will ensure continuity & commitment from caregivers, safety for person, eradicate ‘competing agendas’, proportional ownership within the process • The Essential Life Plan is a ‘Living Document’, alive and accurate at ALL times • Ensure a numbered and descriptive ‘contents page’ include appendix pages e.g. leaflets about the disorder or illness, charts, G.P. consent form, family ‘rogues gallery (pictures & facts) etc.
ESSENTIAL PARTS OF PLAN> • The ‘Complete Person’ approach • List of contributors and/or contacts • Contents page with headings • Approval/consent letter from family GP about any medical issues • Always date pages and any revised pages (for cross ref)
ESSENTIAL PARTS OF PLAN> • Overview of person and condition (A4 double sided for laminating) • Ensure comprehensive ‘Areas of Risk’ • Include persons> likes and dislikes • Include persons> ‘way of being’ • Include necessary Appendix (as many as necessary)
CRUCIAL FOR ‘LIVING DOCUMENT’> • Ownership & Outcomes belong to the person • Belief by all caregivers that the holder (person) is THEexpert in their own experiences (we can choose how to respond to the experience – but not the experience itself) • Plan should be shaped, influenced, directed by the person whenever possible (discuss/read contents with person) • Plan needs a constant source (champion) to accept responsibility for> collating, forming, maintaining, disseminating, updating> ensures plan is a ‘Living Document’ that mirrors the person & their life • The plan offers a vital reference for others should the constant source be unavailable e.g. environment//illness
WHAT CAN SABOTAGE THE PLAN? • Lack of respect for the worth of the person • Empty words lacking meaning (e.g. person centred / holistic etc) • Caregivers ‘not playing’ (gaps within continuum) • Prescriptive models of care which overshadow or diminish plan (from government, agencies, etc)
WHAT CAN SABOTAGE THE PLAN? • Breakdown in continuity (contents, contribution, distribution> should flow between named key players) • Competing or hidden agendas • Reluctance to ‘unlearn’ • Lack of trust in ‘Complete person’ approach • Power games
ADDITIONAL PATHWAYS FOR COMMUNICATION> • DAY DIARY accompanies person to day centre/respite (sharing of info include person) • BULLET POINT UPDATES (for respite unit – staff role limited due to lack of continuous care) • MORE DETAILED THE NEED – THE MORE NEED FOR DETAIL (COMMUNICATE!) • NO ONE CARES HOW MUCH YOU KNOW – UNTIL THEY KNOW HOW MUCH YOU CARE!
PROFILE HELLO MY NAME IS SUSIE ABOUT ME> I am 27 years old (d.o.b. 8:5:80) I am a young woman who has profound learning disabilities and complex and multiple health needs and challenging behaviour. I have a disorder called Rett Syndrome which afflicts at least 1 in every 12,000 of FEMALES. Although I have profound disabilities and have limited cognitive understanding, I have limitless emotional understanding and a strong personality and I find ways of letting others know how I feel, usually by my behaviour and way of being. My dad calls me “an angel with attitude”. ABOUT MY FAMILY> I live at home with my family> mum (Isobel) dad (Dave) and my cat (Meg) plus lots of fish in my fish tank. I have two older brothers who live near. Stephen is 37 years old and lives with his partner Karen and their son Ewan. Scott is 32 years old and has two children, Zoe and Marc. We are your ordinary family > we fight sometimes, we are happy sometimes, we like each other sometimes andlove each other most times. Revised and updated as appropriate
WHOSE LIFE IS IT ANYWAY!