Download
1 / 1
70 likes | 270 Views
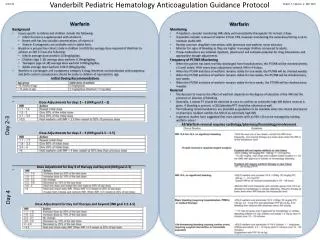
Vanderbilt Pediatric Hematology Anticoagulation Guidance Protocol . 4 / 11 / 12. Robert F. Sidonio, Jr. MD, MSc . . Enoxaparin Dosing Goal anti- Xa levels are 0.6 – 1 units/ mL.

E N D
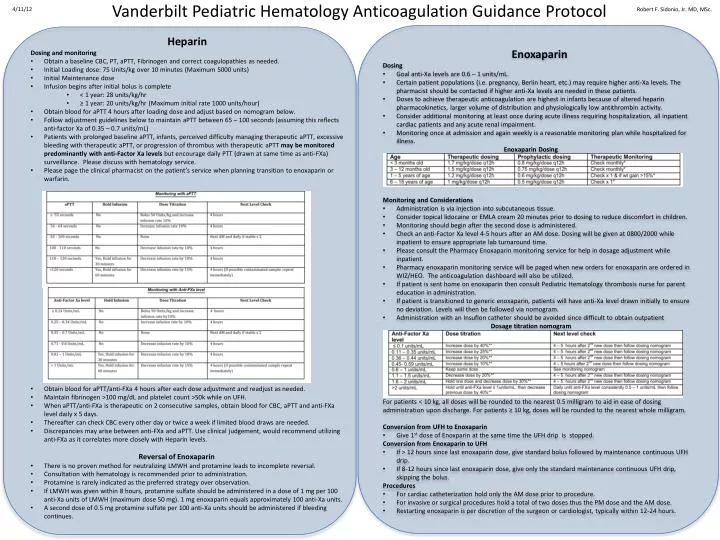
Vanderbilt Pediatric Hematology Anticoagulation Guidance Protocol 4/11/12 Robert F. Sidonio, Jr. MD, MSc. • Enoxaparin • Dosing • Goal anti-Xa levels are 0.6 – 1 units/mL. • Certain patient populations (i.e. pregnancy, Berlin heart, etc.) may require higher anti-Xa levels. The pharmacist should be contacted if higher anti-Xa levels are needed in these patients. • Doses to achieve therapeutic anticoagulation are highest in infants because of altered heparin pharmacokinetics, larger volume of distribution and physiologically low antithrombin activity. • Consider additional monitoring at least once during acute illness requiring hospitalization, all inpatient cardiac patients and any acute renal impairment. • Monitoring once at admission and again weekly is a reasonable monitoring plan while hospitalized for illness. • Enoxaparin Dosing • Monitoring and Considerations • Administration is via injection into subcutaneous tissue. • Consider topical lidocaine or EMLA cream 20 minutes prior to dosing to reduce discomfort in children. • Monitoring should begin after the second dose is administered. • Check an anti-Factor Xa level 4-5 hours after an AM dose. Dosing will be given at 0800/2000 while inpatient to ensure appropriate lab turnaround time. • Please consult the Pharmacy Enoxaparin monitoring service for help in dosage adjustment while inpatient. • Pharmacy enoxaparin monitoring service will be paged when new orders for enoxaparin are ordered in WIZ/HEO. The anticoagulation dashboard will also be utilized. • If patient is sent home on enoxaparin then consult Pediatric Hematology thrombosis nurse for parent education in administration. • If patient is transitioned to generic enoxaparin, patients will have anti-Xa level drawn initially to ensure no deviation. Levels will then be followed via nomogram. • Administration with an Insuflon catheter should be avoided since difficult to obtain outpatient • Dosage titration nomogram • For patients < 10 kg, all doses will be rounded to the nearest 0.5 milligram to aid in ease of dosing administration upon discharge. For patients ≥ 10 kg, doses will be rounded to the nearest whole milligram. • Conversion from UFH to Enoxaparin • Give 1st dose of Enoxparin at the same time the UFH drip is stopped. • Conversion from Enoxaparin to UFH • If > 12 hours since last enoxaparin dose, give standard bolus followed by maintenance continuous UFH drip. • If 8-12 hours since last enoxaparin dose, give only the standard maintenance continuous UFH drip, skipping the bolus. • Procedures • For cardiac catheterization hold only the AM dose prior to procedure. • For invasive or surgical procedures hold a total of two doses thus the PM dose and the AM dose. • Restarting enoxaparin is per discretion of the surgeon or cardiologist, typically within 12-24 hours. • Heparin • Dosing and monitoring • Obtain a baseline CBC, PT, aPTT, Fibrinogen and correct coagulopathies as needed. • Initial Loading dose: 75 Units/kg over 10 minutes (Maximum 5000 units) • Initial Maintenance dose • Infusion begins after initial bolus is complete • < 1 year: 28 units/kg/hr • ≥ 1 year: 20 units/kg/hr (Maximum initial rate 1000 units/hour) • Obtain blood for aPTT 4 hours after loading dose and adjust based on nomogram below. • Follow adjustment guidelines below to maintain aPTT between 65 – 100 seconds (assuming this reflects anti-factor Xa of 0.35 – 0.7 units/mL) • Patients with prolonged baseline aPTT, infants, perceived difficulty managing therapeutic aPTT, excessive bleeding with therapeutic aPTT, or progression of thrombus with therapeutic aPTTmay be monitored predominantly with anti-Factor Xa levels but encourage daily PTT (drawn at same time as anti-FXa) surveillance. Please discuss with hematology service. • Please page the clinical pharmacist on the patient’s service when planning transition to enoxaparin or warfarin. • Obtain blood for aPTT/anti-FXa 4 hours after each dose adjustment and readjust as needed. • Maintain fibrinogen >100 mg/dL and platelet count >50k while on UFH. • When aPTT/anti-FXa is therapeutic on 2 consecutive samples, obtain blood for CBC, aPTT and anti-FXa level daily x 5 days. • Thereafter can check CBC every other day or twice a week if limited blood draws are needed. • Discrepancies may arise between anti-FXa and aPTT. Use clinical judgement, would recommend utilizing anti-FXa as it correlates more closely with Heparin levels. • Reversal of Enoxaparin • There is no proven method for neutralizing LMWH and protamine leads to incomplete reversal. • Consultation with hematology is recommended prior to administration. • Protamine is rarely indicated as the preferred strategy over observation. • If LMWH was given within 8 hours, protamine sulfate should be administered in a dose of 1 mg per 100 anti-Xa units of LMWH (maximum dose 50 mg). 1 mg enoxaparin equals approximately 100 anti-Xaunits. • A second dose of 0.5 mg protamine sulfate per 100 anti-Xa units should be administered if bleeding continues.