Download
1 / 28
280 likes | 399 Views
Indianapolis Discovery Network for Dementia September 2011. Alzheimer’s Disease Multiple Intervention Trial (ADMIT). Funded by the National Institute on Aging R01 AG034946 Performance Dates: July 2010-June 2015. Outline. Update on IU Center for Aging Research

E N D
Indianapolis Discovery Network for Dementia September 2011 Alzheimer’s Disease Multiple Intervention Trial(ADMIT) Funded by the National Institute on Aging R01 AG034946 Performance Dates: July 2010-June 2015
Outline • Update on IU Center for Aging Research • Review of PREVENT (precursor to ADMIT) • Overview of ADMIT • Discussion
IU Center for Aging ResearchPrimary Research Themes • Aging Brain • Late life depression • Dementia • Delirium • Models of Care • GRACE, Healthy Aging Brain Center, House Calls for Seniors • Take Charge Lite (weight gain prevention) • Self-Management • Palliative and End-of-Life Care
Primary Research Faculty • Greg Arling, PhD • Malaz Boustani, MD • Chris Callahan, MD • Noll Campbell, PharmD • Dan Clark, PhD • Su Gao, PhD • Hugh Hendrie, MB, ChB • Siu Hui, PhD • Babar Kahn, MD • Michael LaMantia, MD • Doug Miller, MD • Greg Sachs, MD • Kevin Terrell, MD • Alexia Torke, MD • Wanzhu Tu, PhD • Kathleen Unroe, MD
Administrative Core Callahan, Director Miller and Boustani, Associate Directors Fultz, Senior Program Manager Buchanan and Munger, Program Managers Enrollment Core Implementation Center Biostatistics Core Biomarker Core Key Research Infrastructure Edward R. Roybal Center (NIA P30) Interventions and Practice Research Infrastructure Program (NIMH R24) Midcareer Patient-Oriented Research Mentoring Award (K24) Implementation Center (Regenstrief Foundation)
ADMIT Study Team • Co-Investigators • Mary Austrom, Malaz Boustani, Su Gao, Hugh Hendrie, Michael LaMantia, Doug Miller, Arlene Schmid • Staff • Mickey Vogel (collaborative care nurse practitioner) • Carrie Morris (project coordinator, occupational therapy intervention) • Eric Wehr, Denisha Ferguson (enrollment, outcomes assessment) • Katie Lane, Raven Carter (data management) • Consultants • Laura Gitlin, PhD • Kostas Lyketsos, MD (Independent Data Safety Monitor)
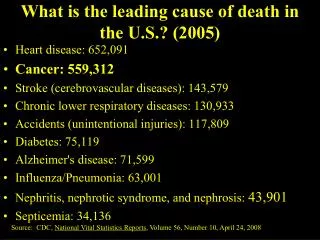
Current Dementia Care Guidelines • Make a diagnosis • Evaluation for treatable causes (including drugs) • Consideration for specialty referral • Patient and caregiver education • Treat reversible comorbid disability • Treatment with cholinesterase inhibitor • Treatment for behavioral disturbances • Coordination of care • Tracking outcomes of care • Support for personal caregiver’s health
Original PREVENT Intervention • One year of care management led by a nurse practitioner working with the patient’s family caregiver and primary care physician • Cholinesterase inhibitor if appropriate • All intervention caregiver’s educated on: • Communication and coping skills • Legal and financial advice • Patient exercise guidelines • Community resources • Referral to Alzheimer’s Association and free enrollment in identity bracelet / safe return program
Original PREVENT Intervention • At each contact, the care manager assessed current problems using symptom checklist • Based on current symptoms, care manager could activate standardized protocols for: personal care delusions sleep disturbance repetitive behavior mobility agitation/aggression depression caregiver health Protocols emphasized non-pharmacologic management
Original PREVENT Intervention • Nurse care manager met with an interdisciplinary support team weekly to review new and/or difficult patients • Patient’s progress monitored with a web-based longitudinal tracking system • Patients seen bimonthly initially and then as needed for one year • Provided ombudsman and problem-solving role for other chronic conditions or navigating health care system
Patient Neuropsychiatric Inventory Scores p < 0.05 p < 0.05 Patient NPI Score Callahan et al. JAMA 2006
Rationale for ADMIT • PREVENT resulted in significant improvement in the quality of care and in behavioral and psychological symptoms for patients and their caregivers. • PREVENT did not slow the rate of patients’ functional decline compared with augmented usual care. • PREVENT did not specifically target functional decline • At least two short-term clinical trials (US and Netherlands) showed efficacy of OT-based interventions in preventing functional decline among subjects with dementia
Care Management by Dementia Care Specialist 24- Hour Crisis Hotline Formal Health Care System Informal Health Care System Community Services Direct medical care for the AD patient by the Dementia Care Team Respite Care Caregiver support and education Home Health Services Ongoing primary care for AD patient by their primary care provider Home-based interventions to delay functional decline Home Modifications Ongoing primary care for family caregiver by their primary care provider Access to a health care Ombudsman or Patient Navigator Alzheimer’s Assoc. Services Local Support Groups Direct medical care for family caregiver by the Dementia Care Team Faith-based Organizations
ADMIT Elevator Speech • ADMIT will test the effectiveness of a comprehensive medical and home-based dementia care management program in preventing functional decline in older adults with dementia • Single blind, randomized controlled clinical trial • Control group receives dementia care management alone • Intervention group receives two years of home-based occupational therapy designed for older adults with dementia
ADMIT STUDY DESIGN HABC Patient with Diagnosis of Dementia Primary Care Patient with Diagnosis of Dementia CSH Patient with Diagnosis of Dementia Informed Consent of Patient and Caregiver Baseline In-Home Assessment Randomization by patient Stratified by Enrollment Site N=90 N=90 Best Practices Primary Care Best Practices Primary Care Plus Home-Based OT Intervention Two-years of active in-home intervention In-home outcomes assessed at 6, 12, 18, & 24 months
What is the Control Condition? • Usual care • Augmented usual care • In-home attention control • PREVENT • PREVENT plus any routine changes • PREVENT as currently implemented at WHS • Best practices including changes over time
What is Best Practices Primary Care? Wishard Health Services Environment IMPACT ACE GRACE HABC Neurology PREVENT ABC-MH Midtown IN-PEACE GRACE PCC + Other Local Studies CSH Others Other National Studies Current Literature House Calls
The Aging Brain Center Medical Home • Nurse practitioner-led collaborative care based in primary care practice • Targets patients with dementia or depression and provide co-management for cardiovascular risks • Support from memory care practice • Linked with community-based service providers • Focus on adequate dose and duration of care • Reduce re-hospitalization
Aging Brain Center Medical Home Regular needs assessment and evaluation of therapy Attention to family caregiver’s health Self-management tools Pharmacological interventions Enhancement of patient’s cholinergic system Medication adherence Reduction in cerebrovascular risk factors Treatment for major depression Management of delirium, pain, and psychosis Care coordination with community resources Modification of the home environment
Occupational Therapy Description • Focus is on preventing or delaying functional decline • Three cycles of intervention over two years • each cycle delivering eight 60-90 minute home sessions • cycle one takes place over 16 weeks • cycle two over 32 weeks • cycle 3 over 52 weeks • Telephone calls take place in intervening weeks • Intervention is tailored to the unique needs and goals of each patient-provider dyad
Caregiver Assessment of Management Problems (CAMP) • What kind of care problems are you having in the morning/afternoon/evening? • What kind of help do you receive? What kind of help do you think you need? • What do you think would make your everyday life easier? • What is a good day like? What is a bad day like? • Are you able to have any time for yourself?
Outcomes Measures • Primary outcome • Alzheimer’s Cooperative Studies Group Activities of Daily Living Scale • Secondary outcomes • Neuropsychiatric Inventory • Short Physical Performance Battery • Short Portable Sarcopenia Measure • MMSE • Word List Learning Test • PHQ-9; GAD-7 (caregiver) • Resource Use Inventory
Timeline Subject accrual began March 2011 rather than January 2011
Key Challenges over Coming Year • Recruitment and expansion of recruitment to other sites • Adequate dose and duration of intervention • Monitoring process of care in both experimental groups • Monitoring changes in the external environment
Discussion • http://iucar.iu.edu