Download
1 / 80
840 likes | 1.23k Views
Organphosphorus Compounds-Induced Neurotoxicity. Mohamed B. Abou-Donia, Ph.D. Department of Pharmacology and Cancer Biology Duke University Medical Center Durham, North Carolina, USA donia@duke.edu 919-684-2221. Organophosphorus compounds .

E N D
Organphosphorus Compounds-Induced Neurotoxicity Mohamed B. Abou-Donia, Ph.D. Department of Pharmacology and Cancer Biology Duke University Medical Center Durham, North Carolina, USA donia@duke.edu 919-684-2221
Organophosphorus compounds Used in medicine, industry, agriculture and as warfare agents. Have a wide range of acute toxicity: a) low acute toxicity chemicals such as tricresyl phosphates (TCPs) b) highly toxic nerve agents such as sarin, soman and tabun.
Actions of Organophosphorus Compounds • Cholinergic Neurotoxicity 2. Organophosphorus Ester-Induced Neurotoxicity (OPIDN) 3. Organophosphorus Ester-Induced Chronic Neurotoxicity (OPICN)
1. Cholinergic Neurotoxicity Inhibition of Acetylcholinesterase (AChE), an enzyme essential for life
+d R R X Organophosphate ORGANOPHOSPHATE
(b) acyl pocket (d) phe 297 phe 295 (c) (a)
Peripheral binding site acyl pocket (d) (b) phe 297 phe 295 (c) (a)
Peripheral binding site acyl pocket (d) (b) phe 297 phe 295 (c) (a)
Manifestations of Organophosphate Poisoning Optic System Pupil Constriction Blurred Vision Lacrimation Brain Headache Dizziness Vertigo Anxiety Apathy Confusion Anorexia Insomnia Lethargy Fatigue Inability to Concentrate Memory Impairment Convulsion Coma Respiratory System Bronchospasm Bronchial Secretion Pulmonary Edema Tightness of Chest Wheezing Cough Difficulty Breathing Gastrointestinal Tract Salivation Nausea Cramps Abdominal Pain Vomiting Diarrhea Fecal Incontinence Cardiovascular System Tachycardia Increased Blood Pressure Musculature Weakness Tremor Fasciculations Twitching Cramps Increased Sweating Urinary - Genital Urinary Incontinence Impotence Uterus Contraction
Treatment of Cholinergic Toxicity 1. 2-PAM (2-pyridine aldoxime methiodide) hydrolyzes phosphorylated enzyme thus accelerating the regeneration of active AChE; should be administered rapidly within 10 to 15 minutes of exposure, before AChE aging. 2. Atropine, an antagonist of muscarinic ACh receptor (AChR)
3. Shielding of AChE Organophosphorus nerve agents,such as sarin act by irreversibly inhibiting AChE in the peripheral and central nervous systems. 2. Pyridostigmine Bromide (PB) is administered to protect against toxicity. PB is approved by the FDA for soman. 3. Prophylaxis Principle is that PB acts by shielding AChE in peripheral nervous system to reversibly inhibit 30-40% of the enzyme, protecting it from permanent inhibition by the nerve gas. 4. Enzyme activity is restored following spontaneous decarbamyalation of the AChE. Result Free enzyme and near-normal neuromuscular an autonomic functions.
4. Bioscavengers • Butyrylcholinesterase (BChE) is a naturally occurring enzyme in blood. 2. Its blood concentration is 2 mg/liter. • BChE has no known function; however, it functions as the first line of defense against poisoning with organphosphorus compounds. • It acts as a bioscavenger, like a sponge to absorb and degrade organphosphorus compounds (e.g., nerve agents and insecticides).
Recombinant BChE (rBCHE) • Recombinant human BChE (rBChE) is being developed under the trade name Protexia® as a pre- and post-exposure therapy for organphosphorus compound poisoning. • Protexia is a pegylated rBChE, that is formed by conjugation of the rBChE with polyethylene glycol in order to: • Decrease rBChE immunogenicity • Increase rBChE stability • Increase circulating serum of rBChE 3. A limited human study of Protexia® has started.
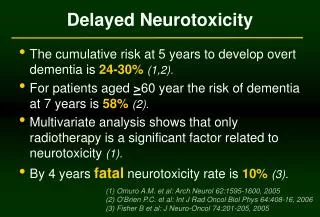
2. OPIDN OPIDN is a neurodegenerative disorder: 1. A latent period; 6 and 14 days. 2. Neuropathological lesions: medulla of the brain, spinal cord, and sciatic nerve. 3. Degeneration of the axon and of myelin 4. Species and age sensitivity. 5. Inhibition of neurotoxicity target esterase (NTE).
+ 3 Phosphorus oxychloride TOCP Synthetic pathways of TOCP Tri-ortho-cresyl phosphate
ortho-cresol meta-cresol para-cresol +POCL3 +POCL3 +POCL3 TOCP TMCP TPCP TCPs
Uses of Tricresyl Phosphates TCPs • Antiwear and additive in synthetic lubricants. • Flame retardant • Plasticizer
Neurotoxity of TCPs • TOCP is a weak inhibitor of AChE • It is a potent producer of OPIDN • Other isomers have not been thoroughly tested for OPIDN
Isomers of Tri-cresyl Phosphate (TCP) There are 10 possible TCP structures: Isomers OPIDN o,o,o + o,o,m; o,o,p + o,m,m,; o,m,p; o,p,p + m,m,m; m,m,p; m,p,p; p,p,p -
Chronology of TOCP-Induced OPIDN Year Country Incidence Cases France Creosote 59 USA Contaminated Ginger Extract Approx. 50,000 1925-1934 France, Germany, Apiol Abortfacient 200-500 Switzerland 1937 South Africa Contaminated Cooking Oil 600 1940 Switzerland Contaminated Cooking oil 80 1942 Britain Manufacturing 3 Britain Contaminated Cottonseed Oil 17 1943-1947 Germany Used as cooking oil 10-20 Switzerland Contaminated food 73 Switzerland Contaminated Olive Oil 80 South Africa Contaminated Water 11 Morocco Used as cooking Oil 10,000 India Contaminated Cooking Oil 58 Rumania Contaminated Alcohol 12 Fiji Islands Contaminated Flower Morocco Shoe Glue Exposure 40 1977-1978 Sri Lanka Contaminated Sesame Oil 23 1988 India Contaminated Cooking Oil 2
Neurological dysfunction of OPIDN Latent period: Days to weeks Progressive phase: Symmetric cramping, numbness and tingling in feet and legs, bilateral dragging of toes (foot-drop), flaccid paralysis. 3.Stationary Phase 4. Improvement Phase: Results from regeneration of PNS; CNS damage becomes unmasked as spasticity and exaggerated knee jerk. 5. Prognosis: Depends on severity of initial symptoms
Factors involved in the Development of OPIDN Chemical Structure Animal Species: Humans are most sensitive Individual differences Animal Age Dose or Concentration at Neurotoxicity Site: a. Exposure dose b. Frequency of exposure c. Duration of exposure d. Route of Exposure e. Other chemical exposure f. Stress
Factors involved in the Development of OPIDN Metabolic Activation: TOCP is activated to saligenin cyclic-o-tolyl phosphate. Phosphorothioate insecticides are activated to phosphates Combined exposure to chemicals that increase activity of CYP 450 enhances TOCP neurotoxicity.
Saligenin cyclic-o-tolyl phosphate TOCP Activation
Factors Involved in the Development of OPIDN Route Of Exposure: Organophosphorus compounds have more access to the nervous system and neurotoxicity target through inhalation and skin penetration than the gastrointestinal tract. Inhalation is the most effective route of entry, preceded only by intravenous injection.
Factors involved in the Development of OPIDN Combined Exposure with other chemicals Chlorpyrifos Propetamphos (safrotin) Oral LD50 in rats 150 mg/kg Causes OPIDN at lethal doses Oral LD50 in rats 119 mg/kg Does not cause OPIDN
3. OPICN Organophosphorus ester-Induced Chronic Neurotoxicity (OPICN) 1. Is a neurodegenerative disorder that results from large toxic or small subclinical doses of Ops. 2. Clinical signs, which continue for weeks to years, consist of neurological and neurobehavioral abnormalities. 3. Damage is greater in the CNS than PNS. 4. Neuronal cell death is seen in various brain areas including cerebral cortex, hippocampal formation and cerebellum. 5. Cell death results from early necrosis or delayed apoptosis. 6. OPICN is exacerbated by concurrent exposure to stress or other chemicals that cause neuronal cell death or oxidative stress. 7. Because CNS injury predominates, improvement is slow and complete recovery is unlikely.
OPICN in the Literature OPICN has been referred to AS: “Chronic neurobehavioral effects” “Chronic organophosphate-induced neuro-psychiatric disorder (COPIND)” “Psychiatric sequelae of chronic exposure” “Psychological and neurological alterations” “CNS system effects of chronic exposure” “Neuropsychological abnormalities” “Long-term effects” “Neurobehavioral effects” “Chronic nervous effects of acute organophosphate poisoning” “Chorea and psychiatric changes” “Delayed neurologic behavioral effects of long-term exposure” “Central cholinergic involvement in behavioral hyperactivity”
Organophosphorus Ester-Induced Chronic Neurotoxicity (OPICN) Individuals exposed to a single large toxic or small subclinical doses of Ops have developed a chronic neurotoxicity that persists years after exposure and is distinct from both cholinergic and OPIDN affects.
Characteristics of OPICN1. Neurological alterations Headache, drowsiness, dizziness, anxiety, increased tension, apathy, restlessness, labile emotions, anorexia, insomnia, bad dreams, weakness, lethargy, fatigue, inability to concentrate, cognitive and memory deficits, depression, social isolation, neurological deficits, irritability, confusion, reduced motor coordination, and tremors. (Not every patient has all of these symptoms)
Characteristics of OPICN2. Neuropathological Changes A large toxic dose of organophosphates produced necrotic neuronal cell death in the following regions of experimental animals: cerebral andpiriform cortices, basal ganglia, thalamus, septum, hypothalamus, hippocampus, corticospinal trac’ and cerebellum. 3. The lesions did not resemble those present in hypoxia or OPIDN.
Characteristics of OPICN2. Neuropathological Changes Exposure to Ops caused delayed apoptotic neuronal cell death in the following regions: Motor cortex Hippocampus Cerebellum and Cervical Spinal cord
Human cases of OPICN 1. Three years and nine months after the Tokyo attack, some victims complained of chronic decline of memory (Nishiwaki et al, 2001). Three years after the Matsumoto attack, some victims complained of fatigue, shoulder stiffness, weakness, blurred vision (Nakajima et al., 1999) 3. Others complained of insomnia, had bad dreams, husky voice, slight fever, and palpitation.
Neuronal cell Death Consequences Significant death of cerebral cortex neurons results in muscular weakness and loss of strength. A loss of significant amount of hippocampal neurons leads to progressive loss of memory and results in learning disabilities. 3. Loss of Purkinje cells in the cerebellum may cause: a. Delays in initiating and terminating movements. b. Terminal tremor at the end of the movement. c. Disorders in the spatial coordination of hand and finger muscle.
Specific Aims This study was designed to investigate the long-term, chronic effects following a single dose of sarin that does not produce clinical signs in male Sprague-Dawley rats.
Experimentals 1. Groups of 15 animals were treated with a single intramuscular injection of sarin (LD50 = 100 μg/kg): a) 1.0 μg/kg (0.01 x LD50) or b) 10.0 μg/kg (0.1xLD50) 2. The following parameters were studied at 24 h, 7 days, one month, and one year. a. Clinical signs b. Neurobehavioral performance c. Brain AChE and plasma BChE activity d. Integrity of the blood brain barrier e. Neuropathological changes in the brain
Clinical Signs 24 Hours, 7 days, one month, one year after Treatment 1. All animals looked and behaved similar to controls. 2. Brain AChE and Plasma BChE activities remained normal 3. Blood brain barrier was intact 4. M2 ACh muscarinic receptor ligand binding was increased in brainstem after one year.
Neurobehavioral Performance Sensorimotor functions were assessed using the following tests: 1. Beam walking and beam score 2. Inclined Plane 3. Forepaw grip time The results showed sensorimotor deficits 3 months after treatment that were exacerbated by the end of the year after treatment.
0,01 and 0.1 x LD50 Sarin after one Year Histological assessments demonstrated neuronal cell death in: 1. Motor cortex 2. Hippocampus 3. Cerebellum and 4. Cervical Spinal cord
Sarin-Induced Apoptosis Apoptosis was confirmed using: 1. Apoptosis-specific stain TUNNL. 2. Neuronal nitric oxide synthase (NOS) immunohistostaining.