Download
1 / 1
10 likes | 143 Views
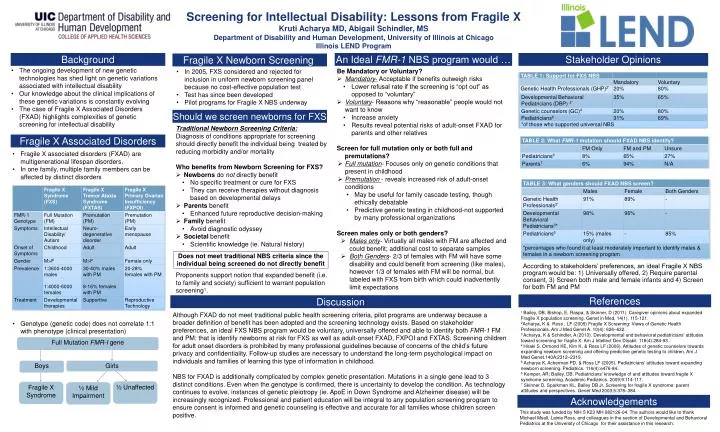
Screening for Intellectual Disability: Lessons from Fragile X Kruti Acharya MD, Abigail Schindler, MS Department of Disability and Human Development, University of Illinois at Chicago Illinois LEND Program . Background. An Ideal FMR-1 NBS program would …. Stakeholder Opinions.

E N D
Screening for Intellectual Disability: Lessons from Fragile X KrutiAcharya MD, Abigail Schindler, MS Department of Disability and Human Development, University of Illinois at Chicago Illinois LEND Program Background An Ideal FMR-1 NBS program would … Stakeholder Opinions Fragile X Newborn Screening • The ongoing development of new genetic technologies has shed light on genetic variations associated with intellectual disability • Our knowledge about the clinical implications of these genetic variations is constantly evolving • The case of Fragile X Associated Disorders (FXAD) highlights complexities of genetic screening for intellectual disability • Be Mandatory or Voluntary? • Mandatory- Acceptable if benefits outweigh risks • Lower refusal rate if the screening is “opt out” as opposed to “voluntary” • Voluntary- Reasons why “reasonable” people would not want to know • Increase anxiety • Results reveal potential risks of adult-onset FXAD for parents and other relatives • Screen for full mutation only or both full and premutations? • Full mutation- Focuses only on genetic conditions that present in childhood • Premutation- reveals increased risk of adult-onset conditions • May be useful for family cascade testing, though ethically debatable • Predictive genetic testing in childhood-not supported by many professional organizations • Screen males only or both genders? • Males only- Virtually all males with FM are affected and could benefit; additional cost to separate samples • Both Genders-2/3 of females with FM will have some disability and could benefit from screening (like males), however 1/3 of females with FM will be normal, but labeled with FXS from birth which could inadvertently limit expectations • In 2005, FXS considered and rejected for inclusion in uniform newborn screening panel because no cost-effective population test • Test has since been developed • Pilot programs for Fragile X NBS underway Should we screen newborns for FXS • Traditional Newborn Screening Criteria: • Diagnosis of conditions appropriate for screening should directly benefit the individual being treated by reducing morbidity and/or mortality • Who benefits from Newborn Screening for FXS? • Newborns do not directly benefit • No specific treatment or cure for FXS • They can receive therapies without diagnosis based on developmental delays • Parents benefit • Enhanced future reproductive decision-making • Family benefit • Avoid diagnostic odyssey • Societal benefit • Scientific knowledge (ie. Natural history) • Proponents support notion that expanded benefit (i.e. to family and society) sufficient to warrant population screening1. Fragile X Associated Disorders • Fragile X associated disorders (FXAD) are multigenerational lifespan disorders. • In one family, multiple family members can be affected by distinct disorders • Genotype (genetic code) does not correlate 1:1 with phenotype (clinical presentation) Does not meet traditional NBS criteria since the individual being screened do not directly benefit According to stakeholders’ preferences, an ideal Fragile X NBS program would be: 1) Universally offered, 2) Require parental consent, 3) Screen both male and female infants and 4) Screen for both FM and PM References Discussion 1 Bailey, DB, Bishop, E, Raspa, & Skinner, D (2011). Caregiver opinions about expanded Fragile X population screening. Genet in Med, 14(1), 115-121. 2Acharya, K & Ross , LF (2009) Fragile X Screening: Views of Genetic Health Professionals. Am J Med Genet A. 10(4): 626–632. 3 Acharya, K & Schindler, A (2013). Developmental and behavioral pediatricians' attitudes toward screening for fragile X. Am J Intellect Dev Disabil. 118(4):284-93.. 4 Hiraki S, Ormond KE, Kim K, & Ross LF (2006). Attitudes of genetic counselors towards expanding newborn screening and offering predictive genetic testing to children. Am J Med Genet.140A:2312–2319. 5Acharya K, Ackerman PD, & Ross LF (2005). Pediatricians' attitudes toward expanding newborn screening. Pediatrics. 116(4):e476-84.. 6Kemper, AR; Bailey, DB. Pediatricians' knowledge of and attitudes toward fragile X syndrome screening. Academic Pediatrics. 2009;9:114-117. 7Skinner D, Sparkman KL, Bailey DB Jr. Screening for fragile X syndrome: parent attitudes and perspectives. Genet Med 2003;5:378–384. Although FXAD do not meet traditional public health screening criteria, pilot programs are underway because a broader definition of benefit has been adopted and the screening technology exists. Based on stakeholder preferences, an ideal FXS NBS program would be voluntary, universally offered and able to identify both FMR-1 FM and PM; that is identify newborns at risk for FXS as well as adult-onset FXAD, FXPOI and FXTAS. Screening children for adult onset disorders is prohibited by many professional guidelines because of concerns of the child’s future privacy and confidentiality. Follow-up studies are necessary to understand the long-term psychological impact on individuals and families of learning this type of information in childhood. NBS for FXAD is additionally complicated by complex genetic presentation. Mutations in a single gene lead to 3 distinct conditions. Even when the genotype is confirmed, there is uncertainty to develop the condition. As technology continues to evolve, instances of genetic pleiotropy (ie. ApoE in Down Syndrome and Alzheimer disease) will be increasingly recognized. Professional and patient education will be integral to any population screening program to ensure consent is informed and genetic counseling is effective and accurate for all families whose children screen positive. Full Mutation FMR-I gene Boys Girls ½ Unaffected Fragile X Syndrome ½ Mild Impairment Acknowledgements This study was funded by NIH 5 K23 MH 082126-04. The authors would like to thank Michael Msall, Lainie Ross, and colleagues in the section of Developmental and Behavioral Pediatrics at the University of Chicago for their assistance in this research.