Download
1 / 27
280 likes | 465 Views
Revision quiz. Musculoskeletal system. Connect the disease and morphology. Acute mastitis Periductal mastitis Lymphocytic mastopathy Fat necrosis. Keratinising squamous metaplasia of the nipple ducts

E N D
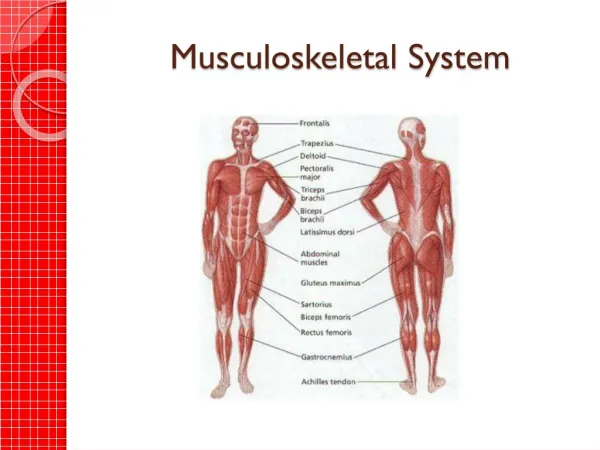
Revision quiz Musculoskeletal system
Connect the disease and morphology • Acute mastitis • Periductal mastitis • Lymphocytic mastopathy • Fat necrosis • Keratinising squamousmetaplasia of the nipple ducts • Single/multiple hard palpable masses; collagenisedstroma surrounding atrophic ducts and lobules • Local infection single/multiple abscesses OR diffuse spreading infection that eventually involves entire breast; neutrophil infiltration, + necrosis • Painless palpable mass or skin thickening/retraction; haemorrhagic with liquefactive fat necrosis
Which lesion is shown in the picture? • Ductal carcinoma in situ • Lobular carcinoma in situ • Invasive carcinoma
Surface protein found on osteoblasts Binds to RANK on the surface of osteoclast progenitors to stimulate differentiation into osteoclasts What is RANKL and what is its function?
Osteoprotegerin Similar to RANK can bind to RANKL Ie. it prevents binding of RANKL/RANK decreases stimulation of osteoclast differentiation Produced by both osteoblasts and osteoclasts What is OPG and what is its function?
Inhibit recruitment and activation of osteoclasts inhibits enzymes on the cell border Promote osteoclast apoptosis it is absorbed by osteoclasts Indirect: stimulate osteoblast activity Eg. alendronate, risedronate What is the MOA of bisphosphonates?
PTH • Vitamin D3 • Calcitonin • Inc Ca2+ absorption, inc phosphate absorption • Inc plasma Ca2+ and dec plasma phosphate • Backup during extreme hypercalcaemia
Name and describe the salter-harris fractures classification
Haematoma formation: fibrin mesh; provides framework for inflammation/fibroblasts Inflammation Formation of a fibrocartilage callus Consolidation: woven bone lamellar bone Remodelling: takes years; continuous alternating resorption/formation What are the stages of fracture healing?
DRABC + compression of bleeding + analgesia + prophylactic a/b Closed reduction Traction Open reduction and internal fixation External fixation Casts splints Functional casts or braces What are the options for first aid/early management of a fracture
# in infant <12 months Avulsion # Metaphyseal # Bucket-handle # Multiple #s of varying ages Bilateral #s Site: posterior rib, scapular, metaphyseal, distal clavicle, spinous processes, sternum Complex skull # What are some indications of a non-accidental injury?
Thicker, strong periosteum with quicker callus formation Inc Haversian canals incomplete fractures; more susceptible to fracturing due to compression Inc cartilaginous bone not seen on x-ray, therefore must infer presence of injury What features affect fractures in children?
Parent: young age, single parent, unwanted pregnancy, poor parenting skills, early exposure to violence, substance abuse, inadequate prenatal care, physical/mental illness, relationship problems Child: sex, prematurity, unwanted, disabled Family: size/density, poor SES, social isolation, high stress levels, Hx of family abuse/domestic violence Community/society: non-existent/unenforced child protection law, dec value of children (minority/disabled/gender), social inequalities, organised violence, high social acceptability of violence, media violence, cultural norms What are some risk factors for child abuse?
Osteoma: benign, from subperiosteal/endosteal surfaces; round-oval fixed tumour of dense sclerotic bone Osteoidosteoma: benign, small painful well-circumscribed; teens/20s Osteosarcoma: malignant mesenchymal tumour; long bone metaphysis; solitary intramedullar tumour with poor differentiation Name 3 bone-forming tumours
Match disease and pathogenesis • Osteogenesisimperfecta • Achondroplasia • Osteoporosis • Osteitisdeformans • Osteomalacia • Osteoclast dysfunction; osteolytic phase mixed phase osteosclerotic phase • Mutated FGF receptor 3 constitutive activation suppressed growth • Deficient synthesis of type I collagen • Defective matrix mineralisation, mostly due to lack of Vit D • Many factors (eg. menopause, aging) affect bone formation after peak bone mass is achieved
Match the knee injury and clinical feature • ACL tear • PCL tear • Medial collateral ligament tear • Meniscal tears • Articular cartilage injury • Knee inflammatory condition • Positive McMurray’s test • Positive Lachman’s test • Knee effusion • Increased laxity with valgus stress • Positive posterior draw test • Knee effusion, pain, fever
Haematogenous (most common) Extension from contiguous site Direct implantation What are the three routes of infection leading to pyogenicosteomyelitis
Pathologic fracture Secondary amyloidosis Endocarditis Sepsis Sarcoma of the infected bone What are the potential complications of chronic osteomyelitis?
Large, destructive, mixed lytic+blastic lesion with permeative margins Sun-ray spicules Tumour frequently breaks through cortex and lifts the periosteum reactive periosteal bone formation What would you see on radiology of an osteosarcoma?
A 49 year old female presents complaining her fingers have been stiff, swollen and sore. What specifically would you ask on history?
She states that it seems to be in both in index fingers and is possibly beginning to affect her right thumb as well. She states that the stiffness is worst in the morning and is relieved by using her hands. She has difficulty writing and knitting. Also generally fatigued.
What is your DDx? What could you find on examination?
Symmetric joint involvement MCP > wrist > PIP > knee > MTP > shoulder > ankle > cervical spine > hip > elbow > TMJ Affected joints: inflammation, swelling, tenderness, warmth, dec ROM Rheumatoid nodules Ulnar deviation of fingers; swan neck or Boutonniere deformities of the fingers, radial deviation at wrist Effects on other joints Potentially extra-articular manifestations