Download
1 / 73
1.01k likes | 3.71k Views
Facial Nerve Paralysis. พ.ท. ขจรเกียรติ ประสิทธิเวชชากูร. Outlines. Anatomy Classification Evaluation Electrodiagnosis testing Management Bell ’ s palsy ,Ramse Hunt syndrome Temporal bone fracture. Anatomy of Facial nerve. The facial nerve contains approximately 10,000 fibers

E N D
Facial Nerve Paralysis พ.ท. ขจรเกียรติ ประสิทธิเวชชากูร
Outlines • Anatomy • Classification • Evaluation • Electrodiagnosis testing • Management • Bell’s palsy ,Ramse Hunt syndrome • Temporal bone fracture
Anatomy of Facial nerve • The facial nerve contains approximately 10,000 fibers • 7000 myelinated fibers innervate the muscles of facial expression, stapedius muscle, postauricular muscles, posterior belly of digastric muscle, and platysma • 3000 fibers form the nervus intermedius (Nerve of Wrisberg) • sensory fibers (taste) from the anterior 2/3 of the tongue • taste fibers from soft palate via palatine and greater petrosal nerve • parasympathetic secretomotor fibers to the parotid, submandibular, sublingual, and lacrimal gland
Anatomy of Facial nerve 1) Intracranial part • Supranuclear segment • Nuclear segment • Infranuclear segment • Cerebellopontine angle • Internal acoustic canal • Labyrinthine segment • Tympanic segment • Mastoid segment 2) Extracranial part
Supranuclear segment • Cerebral cortex Corticobulbar tract Facial nucleus (pons) • Upper face crossed & uncrossed • Lower face crossed only
Nuclear segment • Facial motor nucleus • lower 1/3 of Pons • abducent nucleus • Out from brain stem at pons recess between olive andinferior cerebellar peduncle
Nervous intermedius • Parasympathetic secretory fibers arise from superior salivatory nucleus • These preganglionic fibers travel to the submandibular ganglion via the chorda tympani nerve to innervate the submandibular and sublingual glands • And to sphenopalatine ganglion via greater superficial petrosal nerve to innervate lacrimal, nasal, and palatine gland
Nervous intermedius • Secretory fibers of lesser superficial petrosal nerve tranverse tympanic plexus, synapse in otic ganglion, and travel via auriculotemporal nerve to innervate parotid gland • Taste fibers from anterior 2/3 of tongue reach geniculate ganglion via chorda tympani nerve and from there travel to the nucleus of the tractus solitarius
Submandibular ganglion Submandibular gland
Infranuclear segment • Cerebellopontine angle • Internal acoustic canal • Labyrinthine segment • Tympanic segment • Mastoid segment
Cerebellopontine angle • The facial nerve and nervus intermedius exit the brain stem at the pontomedullary junction and travel with CN VIII to enter the internal acoustic meatus
Internal acoustic canal • Motor facial nerve (medial) • Nervus intermedius (between) • Acoustic nerve (lateral)
Labyrinthine segment • Fallopian canal • Shortest & Narrowest part • Temporal bone • Facial nerve enter fallopian canal until middle ear • First genu • Geniculate ganglion • Branches • Greater superficial petrosal nerve lacrimal gland • Lessor superficial petrosal nerve parotid gland
Tympanic segment • Firstgenu above oval window stapes • Second genu beyond middle ear • Out of cranium through stylomastoid foramen
Mastoid segment • Stylomastoid foramen • Branches • Motor nerve to stapedius muscle • Chorda tympani nerve betweenmalleus andincus • secretomotor : Submandibular & Sublingual gland • taste fiber : anterior 2/3 of tongue
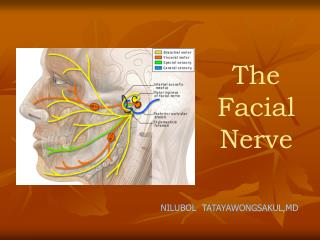
Extracranial segment • Posterior auricular nerve : auricularis, occipitalis and sensation at auricular, post auricular area • Branch to posterior belly of digastric muscle and stylohyoid muscle • Temporal branch: muscle above zygoma • Zygomatic branch : orbicularis occli • Buccal branch : buccinator and upper lip • Marginal mandibular branch : orbicularis oris andlower lip • Cervical branch : platysma
Physiology • Efferentfibers: from the motor nucleus innervate muscles of facial expression, post-auricular, stylohyoid, posterior digastric, and stapedius muscles • Efferentfibers : ANS (preganglionic parasympathetic fiber) • sphenopalatine ganglion to lacrimal glands and mucinous glands of nose • submandibular gangliontosubmandibular and sublingual glands
Physiology • Afferentfibers convey taste from anterior two-thirds of tongue to nucleus tractus solitarius via lingual nerve, chorda tympani, and nervus intermedius. • Afferent fibers mediate sensation from posterior external auditory canal, concha, ear lobe, and deep parts of face
Classificationsof facial nerve injury Seddon classification of nerve injury • Neuropraxia • Axonotmesis • Neurotmesis
Classifications Sunderland classification of nerve injury 1° damage = Compression 2° damage = Interruption of axoplasm 3° damage = Disruption of myelin 4° damage = Disruption of perineurium, myelin and axon 5° damage = Transection of nerve
Nerve injury • neurapraxia ~ Sunderland grade 1 • axonotmesis ~ Sunderland grade 2-3 • neurotmesis ~ Sunderland grade 4-5
Degeneration • Interruption of the continuity of the axon separates the distal axon from its metabolic source, the neuron or cell body • Wallerian degeneration of the distal axon and myelin sheath begins within 24 hours • Macrophages phagocytose degraded myelin and axons
Regeneration • Complete • Partial • Simple misdirection • Clinical expression: synkinesis or associated movement • Complex misdirection • Clinical expression: mass movement
Differential Diagnosis • Extracranial • Intratemporal • Intracranial
Extracranial 1.Traumatic • Facial lacerations • Blunt forces • Penetrating wounds • Mandible fractures • Iatrogenic injuries • Newborn paralysis
Extracranial 2.Neoplasm • Parotid tumors • Tumors of the external and middle ear • Facial nerve neurinomas • Metastatic lesions 3.Congenital absence of facial musculature
Intratemporal 1.Traumatic • Fractures of petrous pyramid • Penetrating injuries • Iatrogenic injuries 2. Neoplastic • Cholesteatoma • Facial neurinomas • Hemangiomas • Meningiomas • Acoustic neurinomas
Intratemporal 3.Infectious • Herpes zoster oticus • Acute otitis media • Chronic otitis media • Malignant otitis externa 4.Idiopathic • Bell's palsy • Melkersson-Rosenthal syndrome 5. Congenital: osteopetroses
Intracranial 1. Iatrogenic injury 2. Neoplastic 3. Congenital • Mobius syndrome • Absence of motor units
History • Onset • Previous symptoms • Complete or incomplete • Unilateral or bilateral • Pain • Underlying disease (vestibulocochlear) • Associate symptoms • Alteration in taste or lacrimation
History • Family history • Trauma • Hx of viral infection • Vaccination • DM • HTN • Pregnancy
Physical examination • ENT exam • Nervous system • Location • Severity
Evaluation of Facial paralysis • Clinical feature • Central VS Peripheral facial paralysis • Complete head and neck examination • Cranial nerve evaluation • Electrodiagnostic testing • Topographic diagnosis
Central facial paralysis • Upper motor neurone lesion • Movements of the frontal and upper orbicularis oculi tend to be spared • Because of uncrossed contributions from ipsilateral supranuclear areas • Involvement of tongue • Involvement of lacrimation and salivation
Peripheral paralysis • Lower motor neurone lesion • At rest : • less prominent wrinkles on forehead of affected side, eyebrow drop, flattened nasolabial fold, corner of mouth turned down • Unable to : • wrinkle forehead, raise eyebrow, wrinkle nasolabial fold, purse lips, show teeth, or completely close eye
House-Brackmann grading system • Grade I- Normal • Grade II- Mild dysfunction, slight weakness on close inspection, normal symmetry at rest • Grade III- Moderate dysfunction, obvious but not disfiguring difference between sides, eye can be completely closed with effort • Grade IV- Moderately severe, normal tone at rest, obvious weakness or asymmetry with movement, incomplete closure of eye • Grade V- Severe dysfunction, only barely perceptible motion, asymmetry at rest • Grade VI- No movement
Topographic Diagnosis • To determine the anatomical level of a peripheral lesion • Lacrimation Geniculate ganglion • Stapedius reflex motor nerve of stapedius muscle • Taste chorda tympani
Schirmer'sTest • Geniculate ganglion & petrosal nerve function test • Schirmer’s test +ve when • Affected side shows less than half the amount of lacrimation seen on the normal side • Sum of the lengths of wetted filter paper for both eyes less than 25 mm • Lesion at or proximal to the geniculate ganglion
Stapedius reflex • Nerve to stapedius muscle test • Impedance audiometry can record the presence or absence of stapedius muscle contraction to sound stimuli 70 to 100 dB above hearing threshold • An absence reflex or a reflex less than half the amplitude is due to a lesion proximal to stapedius nerve
Taste (Electrogustometry) • Chorda tympani nervetest • Solution of salt, sugar, citrate, quinine or Electrical stimulation • Compares amount of current require for a response each side of tongue • Normal : difference < 20 uAmp(thresholds differening by more than 25%= abnormal) • Total lack of Chorda tympani : No response at 300 uAmp • Disadvantage : False +ve in acute phase of Bell’s palsy
Minimal stimulation test • ใช้กระแสไฟฟ้าเปลี่ยนไปเรื่อย ๆ จนได้ ค่าที่น้อยที่สุด ที่สามารถทำให้เห็นกล้ามเนื้อใบหน้ากระตุก • การตรวจวิธีนี้อาศัยหลักเกณฑ์ • neurapraxia ใยประสาทที่อยู่ใต้ต่อรอยโรคสามารถนำกระแสไฟฟ้าได้ดี • axonotmesis ใยประสาทที่อยู่ใต้ต่อรอยโรคยังคงสามารถถูกกระตุ้นด้วยไฟฟ้าได้แต่ต้องใช้ปริมาณกระแสเพิ่มขึ้น • neurotmesis ใยประสาทไม่สามารถนำกระแสไฟฟ้าได้
Minimal stimulation test • ขั้นแรกใช้กระแสไฟฟ้าจำนวนน้อยกระตุ้น • แล้วค่อย ๆ เพิ่มกระแสขึ้นจนได้ค่าน้อยที่สุดที่สามารถทำให้กล้ามเนื้อกระตุกใบหน้ากระตุกได้ • ทำทีละข้างของใบหน้า • เปรียบเทียบค่าที่ได้ของข้างที่มีรอยโรคกับข้างปกติ • ถ้าค่าต่างกันมากกว่า 3.5 mA Wallerian degeneration