Download
1 / 45
1.06k likes | 4.93k Views
The Facial Nerve. NILUBOL TATAYAWONGSAKUL,MD. Anatomy of the facial nerve. 1 . Intracranial. 2 . Intratemporal. 3 . Extratemporal. Anatomy. Intracranial portion. ตั้งแต่ motor cortex จนถึง cerebellopontine angle ก่อนเข้า internal auditory canal. - supranuclear pathway.

E N D
The Facial Nerve NILUBOL TATAYAWONGSAKUL,MD
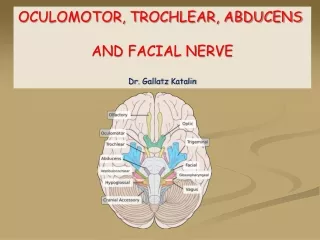
Anatomyof the facial nerve 1. Intracranial 2. Intratemporal 3. Extratemporal
Anatomy Intracranialportion ตั้งแต่ motor cortex จนถึง cerebellopontine angle ก่อนเข้า internal auditory canal - supranuclear pathway - facial nucleus - infranuclearpathway
- contralateral lower face palsy - upper motor neurone lesion - lower motor neurone lesion - ipsilateral whole face palsy
Intratemporal portion - meatal segment - labyrinthine segment - tympanic or horizontal segment - mastoid or vertical segment
Intratemporal portion Meatal segment อยู่ใน IAC content ใน IAC ประกอบด้วย facial nerve, cochlear nerve, superior vestibular nerve, inferior vestibular nerve, labyrinthine artery - Bill's bar (crista falciformis) - Transverse crest.
Intratemporal portion Labyrinthine segment • from fundus of IAC to • geniculate ganglion • between labyrinth and cochlear • 1st branch - greater superficial • petrosal nerve (GSPN) lacrimal, palatine, minor salivary gland - no vascular anastomosis
Intratemporal portion Tympanic or horizontal segment - from genicalate gg to oval window (1st genu to 2nd genu) - no branch -most dehiscence (50%)
Intratemporal portion Mastoid or vertical segment 2 nd genu to stylomastoid foramen - branch to stapedial muscle - chorda tympani nerve submandibular, sublingual gland
Extratemporal or parotid segment - from stylomastoid foramen เข้าสู่ parotid gland แบ่งเป็น superficial and deep lobe แตกแขนงมีลักษณะเป็น pes ancerinus (goose's foot)
Locate most medial aspect of tympanomastoid fissure & between mastoid tip – EAC • at 1-1.5 cm anterior & deep to tragal pointer • Then separate into 3 division at pes anserinus
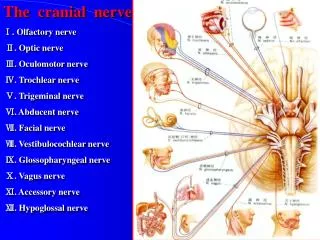
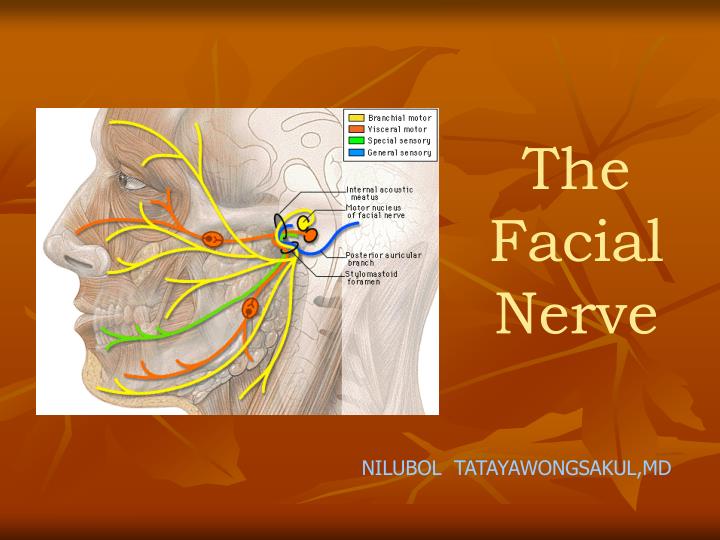
Function of the facial nerve 1. Special visceral afferent (SVA) 2. General visceral afferent (GVA) 3. Special visceral efferent (SVE) 4. General visceral efferent (GVE)
1. Special visceral afferent (SVA) taste fiber (taste bud ant r 2/3 of tongue, hard and soft palate) geniculate gg chorda tympani (lingual nerve) nervus intermedius nucleus of tractus solitareus
2. General visceral afferent (GVA) sensory fibers (tympanic cavity, tympanic membrane, EAC) nucleus of tractus solitareus
3. Special visceral efferent (SVE) motor fiber muscles of facial expression, platysma m., posterior belly of digastric m, stylohyoid m.
4. General visceral efferent (GVE) parasympathetic fiber จาก superior salivary nucleus lacrimal, palatine, minor salivary gland (GSPN) submandibular, sublingual gland (chorda tympani n.)
Pathophysiologyof peripheral nerve lesion Sunderland classification 1st degree (neurapraxia) 2nd degree (axonotemesis) 3rd degree 4th degree neurotemesis 5th degree
Sunderland classification 1st degree (neurapraxia) =compression ทุกอย่างยังดี 2nd degree (axonotemesis) = wallerian degeneration neurotemesis 3rd degree = axon + endoneurium ขาด 4th degree= axon + endoneurium + perineurium ขาด 5th degree = axon + endoneurium + perineurium + epineurium ขาด
House-Brackmann System of grading facial nerve recovery
House-Brackmann System of grading facial nerve recovery
Regeneration of nerve injury Electrical testing can distinguish class I from class II to V lesions but cannot distinguish class II from class V
Special facial nerve test - Topographic test - Prognostic test or Electrical test
Topographic test - Location of facial nerve injury • Test branch of facial nerve • Lacrimation • Salivation • Taste • Stapidius reflex ได้ผลค่อนข้างถูกต้องในราย temporal bone fracture (complete focal lesion) แต่ใน Bell’s palsy จะเชื่อถือได้น้อย(partial lesion with varying degree of conductive block)
Topographic test 1. Lacrimation test=Schirmer’s test
Topographic test 2. Stapedial reflex test
Topographic test 3.Taste test (electrogustometry)
Topographic test 4.Salivary flow test
Topographic test5.Salivary PH • Normal: PH .>,= 6.4 • PH < 6.1= incomplete recovery in case of Bell’s palsy • Accuracy prediction = 91% • Unknown cause this test • Give an earier prognosis than other test
Prognostic test or Electrical test • severity of axonal degeneration • Require serial testing • Compared with the normal side • ใช้access motor function of facial n. at distal to stylomastoid foramen • กรณีlesionที่ proximal กว่าตำแหน่ง test ต้องรอ wallerian degeneration ก่อน test ซึ่งใช้เวลาอย่างน้อย 72 ชั่วโมง(Not determine in the immediate post injury stete)
Electrical test 7 test • Nerve excitability test (NET) or Hilger's test • Maximum stimulation test • Electroneuronography (ENOG) • Evoked Electromyography (EEMG) • Electromyography (EMG • Magnetic stimulation • Facial Nerve Monitoring
Nerve excitability test (NET) or Hilger's test • ใช้ DC current กระตุ้น nerve trunk นาน 0.3msec. เปรียบเทียบ muscle contraction 2 side • ทำหลัง onset 3 day • มักทำ marginal mandibular branch เพราะตื้นที่สุด • Stimulating electrode is place on skin over stylomastiod foramen or over one of peripheral branch of the nerve
Frontal branch - 1 inch lateral to outer canthus Zygomatic branch - bony lateral border of orbit ant r to the point that facial a. pass mandible Marginal mandibular branch –
Nerve excitability test (NET) or Hilger's test • minimum electrical stimulation • > 6mA in injury side - different > 3.5 m A Severe degeneration
NET • เมื่อใช้ NET different >3.5 เป็น criteria ในการทำการผ่าตัด nerve decompression จะมี accuracy 80% • มีประโยชน์เฉพาะ(Useful only) first 2-3 weeks of complete paralysis,before complete degeneration has occure • ใน incomplete paralysis จะมี normal response เมื่อกระตุ้น distal ต่อ pathologic site จึงไม่ควรทำ NET ใน incomplete paralysis • Clinical recovery จะมาก่อน NET recovery จึงไม่มีประโยชน์ในการ F/U NET
Maximum stimulation test (MST) • กระตุ้นด้วย maximal DC current ที่ผู้ป่วยทนได้(5mA) จนเห็น maximal movement • เริ่มทำในข้างที่ดีก่อนแล้วทำข้างเสีย เปรียบเทียบเป็น % กับข้างดี • Stimulate all intact axon,ประเมินสัดส่วนของ fiber ที่ degenerate ฉะนั้นจึงให้information more reliably guide prognosis and treatment than NET (full muscle contraction or pain) • result - equal 100%, mild 75%, moderate 50%, • severe 25%, complete 0% - ถ้า severe (<25%) 75% incomplete recovery
Bell’s palsy ถ้าพบ • Normal MST 88% = complete recovery • Absence of electrically stimulated movement asso. C incomplete recovery
Electroneuronography (ENOG) Evoked Electromyography (EEMG) • หลักการเหมือน MST แต่ recod เป็นกราฟ • Electrical summation potential • เป็น objective test • เป็น most acceptable for • prognostic indicator - เปรียบเทียบ compound action potential (CAP) กับข้างดี
Normal ต่างกันน้อยกว่า 3% • อาจมี Test error 20% • 0-50% degeneration : good prognostic indicator • 50-90% degeneration : fair recovery • >90% degeneration : poor recovery (surgery is indicate in traumatic) • ปัจจุบันใช้ 95% degenertion ( =5% normal site)เป็น surgical indication ใน Bell’palsy (เพราะ ใน 2 wk. จะมี 50% change of poor recovery)
ทั้ง NET, MST, ENOG จะทดสอบได้ก็ต่อเมื่อมี axon degeneration ก่อน ซึ่งจะเกิดขึ้น 48-72 ชม. หลัง injury เพราะฉะนั้นตรวจและแปลผลได้ เมื่อเกิน 72 ชม. ไปแล้ว
Electromyography (EMG) • ใช้ evaluate the motor unit • ใช้ electrode วัด electrical activity • Recoding of spontaneous and voluntary muscle potential by needle introduced into the muscle
Electromyography (EMG) Muscle electrical response at rest and contraction Normal - needle insertion - muscle contraction - rest - no muscle activity - contraction - muscle activity (CAP) Degeneration - fibrillation wave - at rest - no muscle activity - contraction พบประมาณ 2 สัปดาห์ หลัง injury
แปรผล • Biphasic or triphasic = normal motor unit • Fibrillation = degeneration (อาจพบได้ตั้งแต่ 10-14 วัน หลังinjury ซึ่งยืนยันว่ามี degeneration จริง • Polyphasic สำคัญ ใช้บอก = regeneration = reinnervation (4-6 weeks after the onset of the paralysis)
Magnetic stimulation - กระตุ้น facial nerve ตั้งแต่บริเวณ geniculate ganglion, internal auditory canal โดยตรง • ข้อดี 2 ข้อ • ทดสอบได้เร็วตั้งแต่เริ่มมี injury , บ่งตำแหน่งรอยโรคได้, • test up 4 days after on set of Bell’s palsy • without pain and discomfort - ยังอยู่ระหว่างการศึกษาถึงประโยชน์ที่ชัดเจน
Facial Nerve Monitoring • Intra-operative monitoring • Audible EMG(needle or surface electrode, monopolar or bipolar stimulation) • At the end of the case the nerve can be stimulated successfully near the brainstem with low currents (0.05-0.1mA), the prognosis for postoperative function is excellent