Download
1 / 59
600 likes | 910 Views
Retroviruses. Retroviruses. Probably the most studied group of viruses in molecular biology!!! Enveloped, positive-strand RNA viruses Unique morphology and replication Replicate through a DNA intermediate by reverse transcriptase (RT). Retroviruses. Baltimore and Temin in 1970

E N D
Retroviruses • Probably the most studied group of viruses in molecular biology!!! • Enveloped, positive-strand RNA viruses • Unique morphology and replication • Replicate through a DNA intermediate by reverse transcriptase (RT)
Retroviruses • Baltimore and Temin in 1970 • RNA-dependent DNA polymerase (reverse transcriptase ) encoded by retroviruses • Retroviruses replicate through an DNA intermediate • This DNA copy of viral genome integrates into host chromosome • This discovery earned the Nobel prize: contradicted the central dogma of molecular biology-genetic information passed from DNA to RNA and then to protein • Here: from RNA to DNA
History • Rous sarcoma virus: solid tumors in chicken • Other cancer causing retroviruses from other animal species (oncogenes) • 1981: first human retrovirus: Human T-lymphotropic virus (HTLV-1) • 1983: Human immunodeficiency virus (HIV)
Oncoviruses:immortalize or transform target cells, A,B,C,D type according to their core and capsid • Lentiviruses:slow viruses associated with neurologic and immunosuppresive disease • Spumaviruses:no disease • Endogenous viruses:transmitted vertically, 1% of human chromosome, in many animal species and humans, one detected in placental tissue which facilitates placental function
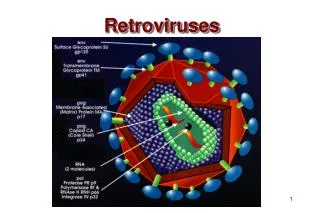
Retroviruses • Enveloped sperical virion • Two copies of positive-strand RNA genome • RT • Provirus integrates randomly into host chromosome • Transcription of the genome is regulated by the interaction of host transcription factors with promoter and enchancer elements in the long-terminal repeat portion (LTR) of the genome
Retroviruses • Simple retroviruses encode gag,pol and env genes • Complex viruses also encode accessory –regulatory genes (tat,rev,nef, vif, vpu for HIV) • Assembles and buds from the plasma membrane • Final morphogenesis requires protease cleavage of gag and gag-pol polypeptides after envelopment.
Gp120 • CD4 surface receptor protein • Initially expressed on cells of the macrophage lineage (macrophage, dendritic cells, microglial cells) (M-tropic)+ second receptor CCR5 • Later on helper T cells (T-tropic) +fusin (CXCR4)
Transmission *Blood, semen,vaginal secretions • Sexual contact • Exposure to contaminated blood and blood products • From infected mother to her baby perinatally
HIV is not transmitted • Casual contact • Touching, hugging, kissing, coughing, sneezing, insect bites, water, food, utensils, toilets, swimming pools, public baths
Transmission • Inoculation of blood: Transfusion, needlesharing among intravenous drug abusers, needlestick, open wound, mucous membrane exposure, tattoo needles • Sexual trasmission: anal and vaginal intercourse • Perinatal transmission: Intrauterine, peripartum and breast milk
Population at high risk • Intravenous drug abusers, sexually active people with many partners (homosexual, heterosexual), prostitutes, newborns of HIV infected mothers • Blood and organ recipients and hemophiliacs: before 1985 (pre-screening programs)
Disease mechanism • HIV primarily infects CD4T cells and cells of macrophage lineage (monocytes, macrophages, alveolar macrophages of the lung, dendritic cells of the skin and microglial cells of the brain • HIV causes lytic infection of CD4T cells and persistant low-level infection of macrophage lineage cells
Disease mechanism • HIV causes syncytia formation, • HIV alters T-cell and macrophage function
Epidemiology • Late 1970s-early1980s • Young homosexual men, Haitians, heroin addicts, hemophiliacs were noted to be dying of normally benign opportunistic infections • HIV appears to have evolved since 1930s from a simian virus and then rapidly spread Africa and the world by an increasingly mobile population. • There is an expanding epidemic worldwide.
Epidemiology Report of UNAIDS (2012): • New infection rate has decreased 50% in 25 UN countries including 13 African countries. Awareness ! • New infections increase in middle east, north Africa,East Europe, Middle Asia
Epidemiology WHO(2012): • 34 milioninfectedwith HIV • 2.5 milionnewinfection • FirstAIDSwasreported in 1985 • HIV/AIDS: 5224(till2011) • HIV/AIDS:1024(in 2012)82% Turkish! • Age:20-60 • Way of transmission : • unknown: 48% • Heterosexual:35.9% • Frominfectedmother:1.1% • Therealnumber !!!!!
AIDS cause by HIV • Retroviridae family • Lentivirinae genus • Enveloped, positive strand RNA virus • 2 identical 9-10kb RNA
AIDS • Human immunodeficiency virus type 1 and 2 (HIV-1, HIV-2)
HIV • HIV-1: isolated in1983 • Responsible from AIDS pandemic • HIV-2: isolated in 1986 • HIV-2 less pathogenic slow progression to AIDS
HIV group and subtypes • Rapid mutation and recombination HIV-1 • Group M (major): A-J • Group O HIV-2 • A-E subtypes
Acute retroviral syndrome • First signs occur in days to several weeks • Transient • %50-70 • Activation of immune system • Multisystem dysfunction • Flu or infectious mononucleosis sydrome like findings • Then a latent period
AIDS • Continuous viral replication • Immune system dysfunction
CD4 T lymphocyes • > 500 /µl (> %29) 1 • 200-499 (% 14-28) 2 • < 200 /µl (< %14) 3
Incubation • Adults with no treatment: 10-11 years • ‘rapid progressors’ : 2-3 years • ‘non-progressor’ : 7-10 years Stable CD4 cell count
HIV genome • Structural genes: gag/env • Pol: enzymes -reverse transcriptase -protease -integrase Tat and Rev: necessary for replication Accessory genes: Vif, Vpr(HIV-1), Vpu, Nef Vpx(HIV-2)
HIV • Viral RNA (in free Virion ) • Viral DNA: integrated in host cell DNA (Provirus)
Seroconversion • Usually 3 weeks • 1.5,3,6,12 months
Laboratory diagnosis Serology: Adults and children older than 15 months: • Initial screening: ELISA, latex agglutination • Confirmation: Western-blot Molecular techniques: -qualitative DNA detection: babies younger than 15 months -quantitative RNA: follow up of HIV infected people who are on therapy
Other tests • Immunologic status: CD4:CD8 ratio Low • Antiretroviral resistance tests
Indicators of disease Opportunistic infections: • Protozoal:Toxoplasmosis • Fungal:Candidiasis, Pneumocystis carinii • Viral :Cytomegalovirus, HSV • Bacterial:Mycobacterium avium-intracellulare Opportunistic neoplasias: Kaposi’s sarcoma
Treatment Nucleoside analaque reverse transcriptase inhibitors: Zidovudine-Azidothymidine(AZT) Dideoxycytidine (DDC) Dideoxyinosine (DDI) d4T(Stavudine) 3TC(Lamivudine) ABC(Abacavir)....
Treatment Non-Nucleoside analaque reverse transcriptase inhibitors: Nevirapine (viramune) Delavirdine(Rescriptor) Efavirez(Sustiva)...
Treatment Protease inhibitors: Saquanavir(Invirase/Fortovase) Ritonavir(Norvir) Indinavir(Crixivan) Nelfinavir(Viracept) Amprenavir(Agenerase)...
Treatment • Binding and Fusion Inhibitors CCR5 inhibitor (maraviroc) T-20 (enfuvirtide/Fuzeon) • Integrase Inhibitor Raltegravir (Isentress)