Download
1 / 62
620 likes | 625 Views
Communication Development in Children with Cochlear Implants. Antonia Brancia Maxon, Ph.D. Diane Brackett, Ph.D. Jennifer Cox, M.A. Alicia Ayles, M.A. Megan Kessler, M.A. New England Center for Hearing Rehabilitation Hampton, CT. EXPECTATION.

E N D
Communication Development in Children with Cochlear Implants Antonia Brancia Maxon, Ph.D. Diane Brackett, Ph.D. Jennifer Cox, M.A. Alicia Ayles, M.A. Megan Kessler, M.A. New England Center for Hearing Rehabilitation Hampton, CT
EXPECTATION • Children who grow up using cochlear implants have the potential to develop superior spoken language skills. • Achievement of that potential is dependent on: • quality of the auditory information (MAP) • dependence on auditory information • input from parents/therapists/children • high expectations
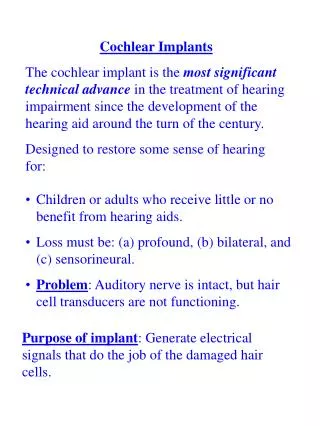
How Cochlear Implants Work • Cochlear implants are designed to bypass damaged hair cells and stimulate the auditory nerve directly through the application of electrical current • The cochlear implant replaces damaged hair cells in the cochlea and does their job for them
UNHS lowers age of intervention • Infants with hearing loss should be fit with hearing aids by four months old at the latest. • Infants with hearing loss should be enrolled in early intervention by four months old at the latest. • Benefit from traditional amplification can be determined by 10 months old at the latest.
UNHS affects the age of cochlear implant candidacy identification • 12 months is recommended lowest age. • Surgeons are implanting even younger infants. • Infants/toddlers who cannot benefit from traditional amplification • degree of loss prevents access to normal conversational level speech with amplification • configuration of loss prevents access to critical speech sounds with amplification
Benefits of Early Cochlear Implantation • Minimizes the effects of auditory deprivation • Electrical stimulation provides necessary information to auditory system at critical period for speech and language acquisition. • Provides child with a good chance to develop normal speech and language
Early Intervention and Language Acquisition • Avoid or decrease potential auditory deprivation that may result in • vocabulary delay (2-3 years at school age) • verbal concepts acquired at slower rate • more concrete language, i.e., difficulty with • multiple meanings • multiple words for same concept • “richness” of vocabulary
Early Intervention and Language Acquisition • Reduce negative impact on initial vocabulary learning • incidental learning • Reduce negative impact on social interaction • idiomatic expressions • slang
Language from Identification to age 3 • Discriminates people’s voices • Discriminates songs • Soothed by the presence of familiar voice • Recognizes many familiar words and phrases • Auditory memory of 2 items in a phrase (Put Elmo on the table.) • Can produce most consonants and all vowels
Language from Identification to age 3 • Understands common verbs • Understands “What” and “Where” questions • Produces sentences with a subject and verb • Uses grammatical forms including plurals (doggies) and present progressive (Doggie is walking) • Likes to sing • Can (and will) repeat back “naughty” words • Speech is intelligible to familiar adults
Age 3 to 5 (home language) • Understands and can attend to longer stories at night • Beginning to use conjunctions, such as “and”. • Understands ‘knock-knock’ jokes • Able to tell stories and ‘tattle’ on siblings, often recounting great detail. • Able to produce more consonants and some ‘blended’ sounds such as /br/
Age 3 to 5 (preschool language) • Can attend to short stories during circle time. • Can follow teacher’s instructions • Can talk with other students, knows when to ask for clarification and when to clarify not understood • Can verbally engage in play • Uses pronouns he/she, him/her • Answers most “WH” questions • Asks “Why?” • Able to follow three step commands
Age 5 to 8 (home language) • Learning how to negotiate verbally (Those cookies sure smell good.) • Adapts to the listener, (changing for stranger, infant vs. adult) • Produces definitions of words when asked • Uses most irregular past tense verbs, such as drank, hid, blew.
Age 5 to 8 (school language) • Is expected to understand instructional language in the classroom, for example, “Put your name at the top of the page in pencil.” • Vocabulary learning becomes more curriculum-based. • Understands non-literal requests • Produces anecdotal narratives • Uses more conjunctions, such as “if”, “but”, “when”
Ages 8 to 11 (social language) • Able to understand the rules of the game (Infield fly rule) • Able to understand the figurative language of sports (Choke up on the bat) • Able to advocate for one’s self when rules or instructions are not heard or understood
Ages 8-11 (school language) • Use of mass nouns (team, troop, class, chorus) • Use of complex verb forms (He could have fallen off the...) • Use of clause structures (If I were walking in the rain I would need an umbrella.) • Able to repair semantic absurdities (The mother read a lullaby to the baby.)
Ages 8 to 11 (school language) • Expected to adjust to the different rules and routines of many teachers • Understands passive voice (The fish was caught by the boy.) • Able to make inferences • Able to use language to compare and contrast (Why or How things are the same or different)
Ages 12-17 (social) • Group conversational skills • 1:1 relationships (intimate language) • Confrontational language • Flirting language • Understanding dating language • Sarcasm/nuance • Clichés • Slang
Ages 12-17 (school) • Interpretation and analysis of information • Hypothesis testing • High level math language • Embedding • Test taking language and procedures • Research and report writing • Driver’s education (language)
NECHEAR Children with Cochlear Implants • Demographic • Number of children = 20 • Bilateral implants = 7 • Additional developmental = 2 • Age at CI = 13 – 108 months • Mean Age = 35.75 months • Therapy = Aural/Oral, Auditory Verbal • School placement = Regular Education • Communication mode = Auditory Oral
Six Years Post-Implant • Test data are presented as mean standard scores (100 = 50th percentile) • All data reflect number of years post-cochlear implant • These data are limited to six years after implantation • All data were obtained through routine annual communication evaluations
Listening Skills • Speech perception assessment • Boothroyd’s Isophonemic nonsense syllables • CVCs • Each list 10 items • Auditory only presentation • Talk-back response
Speech Production • Single word and connected speech • > 5 years: 100% single word, 95% connected • < 5 years: single word - age appropriate, e.g., w/r, w/l, interdental lisp, all produced fricatives • 1 child with oromotor problems – 90% single word, 70% connected speech
Vocabulary Test • Peabody Picture Vocabulary (PPVT) • Receptive single word: nouns, verbs, adjectives, adverbs • Picture point 1 out of 4 items • Expressive Vocabulary Test (EVT) • Expressive single word: nouns, verbs, adjectives, adverbs • Label pictures – provide synonym for picture and given label
Syntax and Figurative Language Tests • CASL (spoken language): multiple subtests • Syntax Construction subtest • e.g., “Here is a bird.” “Here _____ (two birds) • Figurative Language subtest • e.g.,” Tom stopped what he was doing when he saw the red light flash on his mother’s face.”
Assessing Auditory Function • Child needs to receive speech at an appropriate useable level with amplification • detection is not enough • have to look across frequencies for access to all speech sounds • speech needs to be received at a level that allows for learning language
Assessing Auditory Function • Child must have good access to • speech at different distances from sound source • speech of others • own speech • Child should be able to alert • to a variety of speech sounds • to a variety of non-speech sounds • at a variety of distances from the sound source
Mapping Audiologist Needs Information: Adjustment Indicators • CHANGES in speech production and/or perception • child can no longer hear or say a sound previously heard/said • says “ee” for “see” • child is substituting one speech sound for another • says “bad” for “dad”
Mapping Audiologist Needs Information: Adjustment Indicators • Changes in speech pattern • sounds “mushy” • drops final consonants • confuses: /p,t,k/, /n,m/, close vowels (/u, o/) • Increase in distortions • /t/ becomes /s/, /st/ for /s/ • Vowels flatten • /ee/ becomes /eh/
Mapping Audiologist Needs Information: Adjustment Indicators • Reduction of syllables in multisyllabic words • Increase in “what?” for “huh?” • asks for more repetition • Changes in response to environmental sounds
Mapping Audiologist Needs Information: Adjustment Indicators • Changes in voice quality • high pitched or “whiny” sound • “breathless” or whispered quality • child’s voice is louder • close to listener • in quiet situations
Mapping Audiologist Needs Information: Adjustment Indicators • Changes in loudness perception • cannot hear sounds could hear before • at a distance or another room • in the car • in noisy situations • child complains of loudness or quality • not louder enough • cannot understand speech well
Mapping Audiologist Needs Information: Adjustment Indicators • Changes in loudness tolerance • facial nerve stimulation • eye twitch, squinting • nystagmus • pain to certain sounds
When to MAP • Mapping should occur at parents’ or therapist’s request • Regularly scheduled appointments do not allow modification as needed • child has to function with a less than optimal map until time of appointment • OK to schedule, but need to get a MAP “on demand”
Rehab Mapping Procedures • Determine what speech perception error pattern exist • General errors • high frequency cues • vowels - particularly F2 • voicing cues • specific errors • voiceless stop confusion • nasal confusion
Applying Concerns and Problems in Rehab Mapping • Determine which electrodes are responsible for frequencies of error vs target • Change MAP parameters to enhance and highlight specific frequency differences that will reduce misperception.
Auditory Sampling • Auditory sampling as part of every rehabilitation session • document development • document progress • document change in performance • document equipment malfunction
Identifying Auditory Behaviors Auditory Skill Sampling (during interaction) OBSERVE: - awareness of environmental sounds (especially those that occur regularly) - distance listening - increase in requests for repetition - awareness of non-directed speech - increase in loudness of partner’s speech (adapt to need)
Identifying Auditory Behaviors Auditory Skill Sampling (specific sounds) detection vs. identification pointing response vs. speech response closed set vs. open set word vs. sentence no context vs. context
(Re)habilitation Needs Training requires a combination of skill development + dependence analytic training + synthetic training perception + meaning bottom-up + top-down feature-oriented + message-oriented
Strategies to promote carryover Integrate listening, speech and language in every activity. Purpose: reinforce auditory feedback loop; replicate normal communication process.
Strategies to promote carryover Load sessions with multiple examples of the target. Purpose: to allow for the most practice possible in a short period of time. If the child only says the target 5 times in 30 minutes, not enough practice has occurred.
Strategies to promote carryover Acoustically highlight specific forms and targets. Purpose: to provide increased auditory access to specific forms.
Strategies to promote carryover Reduce level of feedback from adult direct modeling to child self-monitoring. Purpose: to reinforce auditory feedback loop; hold child accountable for accurate production and use.
Strategies to promote carryover Reverse roles so that child has to say something to get the adult to do something. Purpose: targets all objective areas simultaneously. Child listens to adult speech and then has to produce clear enough speech for the adult to complete the same task.
Strategies to promote carryover Ask child to repeat what he/she has heard during auditory training activities. Purpose: speech practice; analysis of exact acoustic information missing.