Download
1 / 10
110 likes | 614 Views
LVH & Heart murmur. Murmur Increased w/ standing Decreased w/ supine leg raising, squatting Markedly increased with Amyl Nitrite * * Don’t try this at home. Cardiomyopathy. Cardiomyopathy Restrictive Dilated Hypertrophic Hypertrophic cardiomyopathy (HC) AKA:

E N D
LVH & Heart murmur • Murmur • Increased w/ standing • Decreased w/ supine leg raising, squatting • Markedly increased with Amyl Nitrite* *Don’t try this at home
Cardiomyopathy • Cardiomyopathy • Restrictive • Dilated • Hypertrophic • Hypertrophic cardiomyopathy (HC) • AKA: • Idiopathic Hypertrophic Subaortic IHSS • ASH
Hypertrophic cardiomyopathy (HC) • Asymmetric abnormal septal growth associated with subaortic obstruction. • Dynamic obstruction • Increases w/ decreased ventricle size • Often presents in 3rd decade but can range from infants –elderly • Etiology ? • Autosomal Dominant
Hypertrophic cardiomyopathy • Symptoms • None –> sudden death • Implicated in sudden death of athletes • Dyspnea, palpatations, angina, syncope
Exam • Can be normal • Signs LVH • Murmur • Harsh crescendo –decrescendo systolic murmur at the apex • Increased w/ standing, tachycardia, Amyl Nitrite, NTG, exercise • Decreased w/ squatting, isometric hand grip, beta blockade
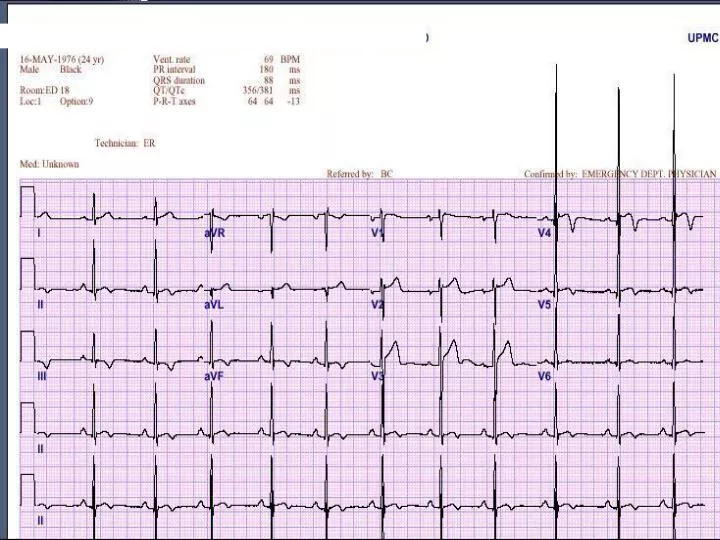
EKG • Pseudoinfarct patterns with noninfarctional Q waves and ST-T-wave changes • “Differentiating the EKG pseudoinfarctional patterns of IHSS from AMI may be impossible. “
Evaluation • Echo • Thalium (may show defects w/ nl coronary arteries) • Cardiac cath
Treatment • Reduce contractility, increase ventricular volume • Beta blockers, Calcium channel blockers • Avoid sports or strenuous activity
Why is this important for us? • Sudden death in a young person is bad • Difficult to predict • Syncope is ominous in kids, not a predictor in adults • HX NSVT is a predictor in adults • Relatives should be evaluated • Avoid certain drugs • Difficult to differentiate from normal hypertrophy seen in athletes