Download
1 / 1
10 likes | 111 Views
Unearthing the True Prevalence of Anxiety Within a Typical DGH Cohort of IBD Patients: Is it Time We Considered Routinely Screening for Anxiety?. N. Swart 1 , D. Wellsted 1 , K. Lithgo 2 , T. Price 2 , M. W. Johnson 2.

E N D
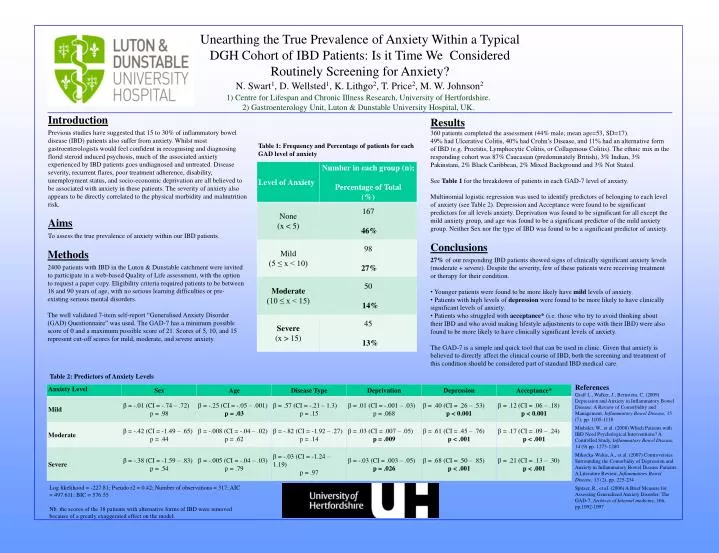
Unearthing the True Prevalence of Anxiety Within a Typical DGH Cohort of IBD Patients: Is it Time We Considered Routinely Screening for Anxiety? N. Swart1, D. Wellsted1, K. Lithgo2, T. Price2, M. W. Johnson2 1) Centre for Lifespan and Chronic Illness Research, University of Hertfordshire. 2) Gastroenterology Unit, Luton & Dunstable University Hospital, UK. Introduction Previous studies have suggested that 15 to 30% of inflammatory bowel disease (IBD) patients also suffer from anxiety. Whilst most gastroenterologists would feel confident in recognising and diagnosing florid steroid induced psychosis, much of the associated anxiety experienced by IBD patients goes undiagnosed and untreated. Disease severity, recurrent flares, poor treatment adherence, disability, unemployment status, and socio-economic deprivation are all believed to be associated with anxiety in these patients. The severity of anxiety also appears to be directly correlated to the physical morbidity and malnutrition risk. Aims To assess the true prevalence of anxiety within our IBD patients. • Results • 360 patients completed the assessment (44% male; mean age=53, SD=17). • 49% had Ulcerative Colitis, 40% had Crohn’s Disease, and 11% had an alternative form of IBD (e.g. Proctitis, Lymphocytic Colitis, or Collagenous Colitis). The ethnic mix in the responding cohort was 87% Caucasian (predominately British), 3% Indian, 3% Pakinstani, 2% Black Caribbean, 2% Mixed Background and 3% Not Stated. • See Table 1 for the breakdown of patients in each GAD-7 level of anxiety. • Multinomial logistic regression was used to identify predictors of belonging to each level of anxiety (see Table 2). Depression and Acceptance were found to be significant predictors for all levels anxiety. Deprivation was found to be significant for all except the mild anxiety group, and age was found to be a significant predictor of the mild anxiety group. Neither Sex nor the type of IBD was found to be a significant predictor of anxiety. • Conclusions • 27% of our responding IBD patients showed signs of clinically significant anxiety levels (moderate + severe). Despite the severity, few of these patients were receiving treatment or therapy for their condition. • Younger patients were found to be more likely have mild levels of anxiety. • Patients with high levels of depression were found to be more likely to have clinically significant levels of anxiety. • Patients who struggled with acceptance* (i.e. those who try to avoid thinking about their IBD and who avoid making lifestyle adjustments to cope with their IBD) were also found to be more likely to have clinically significant levels of anxiety. • The GAD-7 is a simple and quick tool that can be used in clinic. Given that anxiety is believed to directly affect the clinical course of IBD, both the screening and treatment of this condition should be considered part of standard IBD medical care. • x Table 1: Frequency and Percentage of patients for each GAD level of anxiety Methods 2400 patients with IBD in the Luton & Dunstable catchment were invited to participate in a web-based Quality of Life assessment, with the option to request a paper copy. Eligibility criteria required patients to be between 18 and 90 years of age, with no serious learning difficulties or pre-existing serious mental disorders. The well validated 7-item self-report “Generalised Anxiety Disorder (GAD) Questionnaire” was used. The GAD-7 has a minimum possible score of 0 and a maximum possible score of 21. Scores of 5, 10, and 15 represent cut-off scores for mild, moderate, and severe anxiety. Table 2: Predictors of Anxiety Levels References Graff L., Walker, J., Bernstein, C. (2009) Depression and Anxiety in Inflammatory Bowel Disease: A Review of Comorbidity and Management, Inflammatory Bowel Disease, 15 (7), pp. 1105-1118 Miehsler, W., et al. (2008) Which Patients with IBD Need Psychological Interventions? A Controlled Study, Inflammatory Bowel Disease, 14 (9) pp. 1273-1280 Mikocka-Walus, A., et al. (2007) Controversies Surrounding the Comorbidiy of Depression and Anxiety in Inflammatory Bowel Disease Patients: A Literature Review, Inflammatory Bowel Disease, 13 (2), pp. 225-234 Spitzer, R., et al. (2006) A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7, Archives of Internal medicine, 166, pp.1092-1097 Log likelihood = -227.81; Pseudo r2 = 0.42; Number of observations = 317; AIC = 497.611; BIC = 576.55 Nb. the scores of the 38 patients with alternative forms of IBD were removed because of a greatly exaggerated effect on the model.