Download
1 / 67
720 likes | 812 Views
Acetylcholine. Has little therapeutic value Has multiple actions Has short t ½ Activates muscarinic & nicotinic receptors. Pharmacodynamics of Ach. Muscarinic stimulation: On the CVS: - ve chronotropic & inotropic effects Decrease stroke volume & cardiac output Decrease ABP:

E N D
Acetylcholine • Has little therapeutic value • Has multiple actions • Has short t ½ • Activates muscarinic & nicotinic receptors
Pharmacodynamics of Ach • Muscarinic stimulation: • On the CVS: • -vechronotropic & inotropic effects • Decrease stroke volume & cardiac output • Decrease ABP: • Stimulation of vascular M3 receptors • Increase NO release from endothelium
Pharmacodynamics of Ach • Eye: • Miosis: • Contraction of circular muscle of iris • Accommodation to near vision: • Contraction of ciliary muscle of the eye • Decrease IOP( intra-occular pressure)
Pharmacodynamics of Ach • Exocrine glands & GI secretion: • Increase secretion • Contraction of intestinal wall & relaxation of sphincters: • Defecation • Contraction of bladder wall & relaxation of sphincter: • Urination
Pharmacodynamics of Ach • Bronchi: • Bronchoconstriction • Increase mucosal secretion • Penile erection: • Increase release of nitric oxide
Pharmacodynamics of Ach • Nicotinic receptor stimulation: • Autonomic ganglia: • Stimulation • Adrenal medulla: • Increase noradrenaline & adrenaline secretion • NM Junction transmission: • Muscle contraction
Cholinomimetics • Mimic or simulate actions of Ach: • Direct-acting • Indirect-acting
Direct acting cholinomimetics • Activate directly cholinergic receptors: • Cholineesters: • Bethanechol, Carbachol, Methacholine • Resist degradation by cholinesterases • Have longer duration of action than Ach • Naturalalkaloid: • Pilocarpine • Acts directly on end organs like the eye
Bethanechol • Derivative of Ach • Has: • Little nicotinic effects • Good muscarinic effects on bladder & GIT • Leads toeasy urination & defecation • Used to treat post-operative or post-labour: • Urinary retention or paralytic ileus: the weakness of intestine to push its content causing constipation because of weak peristaltic activity
Carbachol • Derivative of Ach • Has muscarinic & nicotinic actions • Limited use: • Because of nicotinic effects on ganglia & adrenal medulla • Used mainly topically as miotic in glaucoma to decrease high intraocular pressure (IOP)
Pilocarpine • Natural plant alkaloid • Resistant to CE enzyme • It produces: • Miosis (contraction of circular muscle of iris) • Contraction of ciliary muscle of the eye • Reduction of IOP • Used topically in glaucoma
Pilocarpine • Lowers high IOP in close-angle & open angle chronic glaucoma • Improves outflow of aqueous humour: • Opens fluid pathway • Increase aqueous flow through canal of Schlemm • Secondary to contraction of circular muscle of the iris & ciliary muscle • Stimulates sweating, lacrimation, salivation
Indications of direct cholinomimetics • Paralytic ileus (Bethanechol) • Urinary retention (Bethanechol) • Glaucoma (Pilocarpine & Carbachol topically • Xerostomia (dry mouth) of Sjogren’s syndrome (oral pilocarpine)
Adverse effects of direct cholinomimetics • Excessive sweating, salivation • Flushing, hypotension • Abdominal colic & diarrhoea • Bronchospasm • Pilocarpine: • Impaired accommodation to far vision & darkness
Contraindications of cholinomimetics • Bronchial asthma • Peptic ulcer
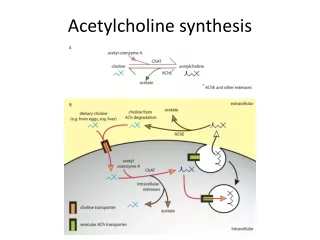
Cholinesterase enzymes • CE is a protein • In cholinergic synapses & RBC • Metabolizes Ach into choline & acetate • Specific for Ach in cholinergic synapses • Pseudocholinesterase in plasma & liver • Not specific to Ach • Metabolizes other drugs (suxamethonium, procaine)
Classification of indirect-acting cholinomimetics Classified into: • Reversible cholinesterase inhibitors • Irreversible cholinesterase inhibitors
Uses of indirect-acting cholinomimetics • Diagnosis of MG (Edrophonium) • Treatment of MG (Pyridostigmine) • Reversible NMB intoxication (Neostigmine) • Alzheimer’s disease (Donepezil) • Irreversible CEI: insecticides
Myasthenia gravis (MG) • Autoimmune (autoantibodies to NM in NMJ) • Reduction in receptor number • Muscle weakness, fatigability,, difficult speaking & swallowing • Treatment: • Reversible CEI • Thymectomy • Immunosuppressant
Reversible ChE inhibitors • Inhibit reversibly CE enzyme • Accumulation of Ach • Electrostatic bonds • Stimulate nicotinic & muscarinic receptors • Useful in myasthenia gravis
Neostigmine • Synthetic CEI, does not cross BBB • Duration of action (4 hrs) • Mainly in MG & also in: • Antidote to competitive NM blocker tubocurarine poisoning • Paralytic ileus, urinary retention • Given orally, SC
Pyridostigmine • Similar to neostigmine • Has longer duration of action (6 hrs) • Useful orally in myasthenia gravis
Cholinergic Crisis: • Over-stimulating of nicotinic receptors can cause muscle weakness and paralysis by the excessive intake ofAnticholinesteraseswhich are (indirect drugs) • Over-stimulation of nicotinic receptors will lead to its blockage instead of further activation. • Cholinergic crisis can happen to myasthenia gravis patients who are overdosing on anticholinesterases drugs.
Edrophonium • Similar to neostigmine • IV, short duration of action (10-20 min) • Useful in diagnosis of MG • To differentiate between weakness due to myasthenic crisis or cholinergic crisis: • Myasthenic crisis improvement • Cholinergic crisis aggravated
Adverse effects of CEI • Excessive salivation • Flushing and hypotension • Abdominal colic and diarrhoea • Bronchospasm
CEI useful in Alzheimer’s disease • Tacrine • Reversible CEI used in treatment of Alzheimer’s disease; • hepatotoxic • Donepezil • New selective CEI • Once daily • Lacks hepatoxicity of tacrine • Useful in Alzheimer’s disease
Irreversible CE Inhibitors • Organophosphorous compounds • Irreversibly inhibit CE • Covalent bond in Enzyme-inhibitor complex • Used as insecticides: • Parathion, malathion • As nerve gases in chemical warfare: • Tabun, Sarin, Soman
Isoflurophate (DFP) • OP compound • Irreversibly inhibits CE • Insecticide • Toxicity: excessive cholinergic stimulation • May be used topically in glaucoma • Duration of action about a week
Echothiophate • New agent • Similar to isoflurophate • Long duration of action (week)
Differences between direct & indirect-acting cholinomimrtics • Actions on receptors: • Direct • Indirect • Pharmacodynamic effects: • Similar • Central effects with indirect: • Cross BBB
Organophosphorous Insecticide Poisoning • Agricultural or industrial accidents • Excessive cholinergic manifestations • GIT (diarrhoea, colic) • Respiratory (dyspnoea, bronchospam) • CV (bradycardia, hypotension) • Micturition, excessive sweating, M. paralysis • Miosis (pin-point pupil), convulsions & death
Treatment of OPI Poisoning • General measures • High doses atropine IV or IM • Mechanical ventilation • Diazepam for convulsions • Enzyme reactivation by pralidoxime IM
Cholinergic Antagonist Drugs • Anti-muscarinic drug: Atropine-like drugs, Hyoscine (Scopolamine) • Anti-nicotinic drugs • Ganglion blockers: Used in experimental pharmacology. E.g. Nicotine, Trimethapan. • Neuro-muscular blockers: Used in surgery to produce complete muscle relaxation.
Anti-muscarinic anti-cholinergic drugs • Natural agents: • Atropine, Hyoscine • Semi-synthetic • Homatropine • Synthetic • Ipratropium, Pirenzepine, Propantheline
Anti-muscarinic • Atropine (Hyoscyamine) • Alkaloids obtained from Atropa Belladona, • Considered as prototype for parasympatolytics • Hyoscine (Scopolamine) • Obtained from Hyocyamus niger plant (Datura Stramonium) Note: Antihistamines, phenothiazides and some antidepressants have anti-muscarinic effects
Clinical pharmacology of anti-muscarinic drugs Mechanism of action: • Reversible blockade of M receptors • Exocrine glands are most sensitive • Gastric secretion is the least affected • Heart is intermediate Note: Atropine blocks all 3 subtypes receptors (M1,M2,M3)
Pharmacokinetics • Absorption: • Natural and most tertiary amines: good • Wide distribution and cross BBB • Quaternary amines: poorly absorbed and poor crossing BBB (Ipratropium) • Atropine t½: 2hrs • Partly metabolized and partly excretedunchanged
Pharmacodynamics • Exocrine glands: at low doses reduced secretions • Salivary • Bronchial • Sweet glands
CNS • Central stimulant effects (Atropine) • Some may produce sedation (Hyoscine) • Hyoscine blocks M receptors in vomiting centre and has anti-emetic effect • Toxic doses: hallucination, convulsion, coma
Eye • Mydriasis (dilatation of pupil) • Cycloplegia (relaxation of the ciliary muscle) cause: blurred vision and impaired accommodation to near vision • Decreased lacrimation • Increase IOP