Download
1 / 20
210 likes | 573 Views
Autoimmune Hepatitis. Seyed Moayed Alavian M.D. Professor of Gastroenterology and Hepatology Director Middle East Liver Disease Center (MELD Center) Editor-in-chief of Hepatitis Monthly E mail: editor@hepatmon.com.

E N D
Autoimmune Hepatitis Seyed Moayed AlavianM.D. Professor of Gastroenterology and Hepatology Director Middle East Liver Disease Center (MELD Center) Editor-in-chief of Hepatitis Monthly E mail: editor@hepatmon.com
Shafiei M, Alavian SM. Autoimmune hepatitis in iran: what we know, what we don't know and requirements for better management. Hepat Mon. 2012 Feb;12(2):73-6.
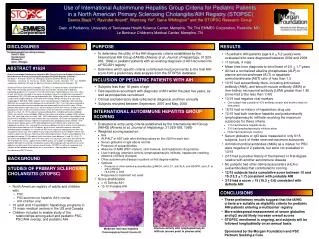
In Iran • The number of Iranian studies published so far about autoimmune hepatitis has been very limited. • Iranian patients with AIH are typically women (male/female: 1:4), usually in their 30s and almost all of them have type 1 Shafiei M, Alavian SM. Autoimmune hepatitis in iran: what we know, what we don't know and requirements for better management. Hepat Mon. 2012 Feb;12(2):73-6. Malekzadeh Z, Haghazali S, Sepanlou SG, Vahedi H, Merat S, Sotoudeh M, et al. Clinical features and long term outcome of 102 treated autoimmune hepatitis patients. Hepat Mon. 2012 Feb;12(2):92-9.
In Iran • Iranian patients with AIH have an excellent 10-year survival rate of 96%, which is consistent with findings from previous studies carried out on other ethnic groups. Shafiei M, Alavian SM. Autoimmune hepatitis in iran: what we know, what we don't know and requirements for better management. Hepat Mon. 2012 Feb;12(2):73-6. Malekzadeh Z, Haghazali S, Sepanlou SG, Vahedi H, Merat S, Sotoudeh M, et al. Clinical features and long term outcome of 102 treated autoimmune hepatitis patients. Hepat Mon. 2012 Feb;12(2):92-9.
The scoring system suggested by the IAIHG lists all the different presentations of this disease and the sum of the scores determines the accuracy of the diagnosis before and after treatment with glucocorticoids. • Apart from the human leukocyte antigen (HLA) typing test and tests for detecting investigational autoantibodies including; the asialoglycoprotein receptor (ASGPR), anti actin, anti LC1 and anti SLA/LP, other tests related to the IAIHG scoring system are routinely available in Iranian laboratories.
Another problem in Iran is the incorrect use of other diagnostic tests related to AIH. • Common mistakes are the evaluation of positive/negative results without consulting the titration of serum autoantibody levels (ALKM-1, ASMA, ANA and AMA) and the incorrect interpretations of these tests.
According to the latest guidelines; titers equal to or more than 1:40 for all the autoantibodies in adults, and in children titers equal to or more than 1:20 for ANA and ASMA and the titers equal to or more than 1:10 for ALKM-1, are considered to be positive and have scoring values. • However, many Iranian medical centers only consider the test positive if the titers are equal to or more than 1:80.
Despite the fact that almost all of the credible references and guidelines recommend a liver biopsy, before the start of treatment for patients who are suspected to have AIH , we still see in Iran, patients that didn’t have any contra-indication to undergoing liver biopsy but treated without it.
Liver biopsy • Liver biopsy plays an important role in establishing a diagnosis of AIH. This is based both on the presence of typical features supporting a diagnosis of AIH and on the absence of atypical features (e.g., biliary abnormalities or steatosis) that might point to an alternative diagnosis. Liver biopsy should be performed to confirm the diagnosis unless there is a good reason or contraindication.
Interface hepatitis PBC Plasma cell infiltration PSC
Up to 20% of patients with proven fatty liver disease based on their liver histology, had the criteria for a definite or probable diagnosis of AIH before undergoing a liver biopsy. • Diagnosing AIH in patients with underlying NASH may be difficult, especially in the presence of a positive ANA.
Extrahepatic Manifestationsup to70% of type 1 patients have immunological Dis • Thyroiditis, or Graves’ dis up to 45% • Celiac sprue • Hemolytic anemia • ITP • Type 1 diabetes mellitus • Ulcerative colitis (more often associated with PSC). • liver disease may predate colitis in the last two
Patients with acute hepatitis are indistinguishable from those seen with acute viral hepatitis • liver biopsy shows changes of underlying chronic liver disease including bridging fibrosis or cirrhosis
Fulminant AIH • The rare patients who present with fulminant AIH often fail to respond to immunosuppression and require liver transplantation. • Although it is worth starting immunosuppressive therapy, it is also important not to delay referral to a transplant center if there is evidence of liver failure as demonstrated by the development of encephalopathy, coagulopathy, or renal failure.
Azathioprine, when to start • Delaying the introduction of azathioprine for 2–3 weeks : • It allows the diagnosis to be confirmed by demonstrating steroid responsiveness before adding in a second immunosuppressive agent • liver toxicity due to azathioprine can be confused with non-responsiveness if azathioprine is started immediately.
All patients on prednisolone at more than 7.5 mg/day should be advised to take calcium and vitamin D supplements or bisphosphonate to prevent osteoporosis.
When to stop therapy • Normalization of liver biochemistry during corticosteroid therapy does not necessarily indicate suppression of histological inflammatory activity—confirmation of histological remission (defined by the absence of interface hepatitis) is therefore recommended before immunosuppressive therapy is withdrawn.
Outcome • The AIH mortality rate is 80% in untreated patients Prednisolone in combination with azathioprine, is the standard treatment. • The treatment prolongs survival and improves clinical, biochemical, and histological features in 65% to 80% of patients. • 10-year survival rate among treated patients may exceed 90%, which is almost identical to that in an age- and sex-matched control population • However, the 20-year survival rate may be less than 80% among patients without cirrhosis and less than 40% among those with cirrhosis at presentation
I would like to emphasize on: • Importance of sooner diagnosis of AIH • Is clinical criteria sufficient? • Is liver biopsy essential? • How much serologic testing is costing? • When do you think about the overlap syndrome? • On time and correct treatment of AIH • Which one of patients should be treated? • What is the preferred protocol? • How do you management of disease on time of treatment? • When do you tapering? • When do you withdrawal of treatment? • How do you follow up after withdrawal? • How do you treatment of relapse disease? • When do you making use of second line of drugs
If you like to receive the PDF free of charge of this book, please send me an e maileditor@hepatmon.com