Download
1 / 17
180 likes | 281 Views
Early Intervention Study. Early Intervention Task Force Members: Carla Tanner, Ed.D., CSC Leslie Gudgel, Laura Dester Shelter, Neonatal Follow Up Clinic Kim Wofford, Parent Advocate; Laura Dester Shelter Suzie Drover, HeadStart Lyn Lucus, Family and Children Services, working with HeadStart

E N D
Early Intervention Study Early Intervention Task Force Members: Carla Tanner, Ed.D., CSC Leslie Gudgel, Laura Dester Shelter, Neonatal Follow Up Clinic Kim Wofford, Parent Advocate; Laura Dester Shelter Suzie Drover, HeadStart Lyn Lucus, Family and Children Services, working with HeadStart Jan Figart, CSC Sherlyn Walton, TARC, Family Support Coordinator Zaida Castro-Kepford, TARC, Hispanic Outreach Specialist Ellen Schmeder, SoonerStart Regional Director Gina Ferman R.N., Regional Coordinator, Sooner Success, University of Oklahoma DeeAnn Brown, Resource and Referral Specialist, CCRC Brenda Butcher, Tulsa Health Department, Child Guidance Program Colleen Ayers-Griffin, Tulsa Healthy Start, CSC Barbara Fyfe, Parent Child Center of Tulsa
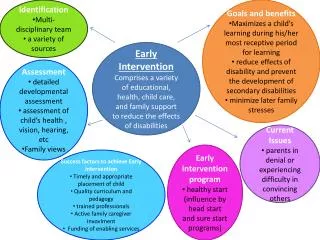
Early Intervention Study • Purpose • Early Intervention Task Force • Target Population
What is Early Intervention? WHAT IS EARLY INTERVENTION? • Early intervention applies to children of school age or younger who are discovered to have or be at risk of developing a handicapping condition. • Early intervention consists of the provision of services that such children and their families may need, to lessen the effects of the condition. WHY IS EARLY INTERVENTION IMPORTANT? • Developmental disabilities are present in 17 percent of American children; with as many as one in eight children having mental retardation and /or a developmental disability. • However, many children with behavioral or developmental disabilities are missing vital opportunities for early identification and intervention.
IS EARLY INTERVENTION COST EFFECTIVE? The available data emphasize the long-term cost effectiveness of early intervention. On a short-term basis, Early Intervention is more costly than traditional school-aged service delivery models. However, there are significant examples of long-term cost savings that result from early intervention programs.
Cost Effectiveness of Early Intervention Perry Preschool Project found that when schools invest about $3,000 for 1 year of preschool education for a child, they immediately begin to recover their investment through savings in special education services.
Early Intervention In Oklahoma Approximately 17% percent of Oklahoma children have a disabling condition. • We identify a small percent of these children early enough to provide an appropriate Early Intervention program. • Sooner Start child count in 2003 was 2.24% of the children birth to 36 months of age. • Tulsa Public Schools enrollment 2003 data indicates that 17 percent of children in elementary schools have a disability. • Less than 50% of the children are identified as having a problem before starting school.
Why is there a disparity? Two factors were identified as contributing to the disparity between estimated populations and those served. • The role played by pediatric practitioners in screening, surveillance, and referral to early intervention services, and • Barriers faced by parents in seeking early intervention services for their children with developmental and/or behavioral delays.
Pediatric Practitionersare a Vital Link • Pediatric Practitioners play a substantial role in identifying children with development and/or behavioral disabilities and referring these children for early developmental intervention. • Historically, however, pediatricians have only been minimally effective as Child Find linkage • Research indicates that physicians often do not conduct regular developmental screening and surveillance • Physicians often adopt a “wait and see” attitude.
DEVELOPMENTAL SURVEILLANCE, SCREENING AND DIAGNOSTIC EVALUATIONS WHAT IS DEVELOPMENTAL SURVEILLANCE AND SCREENING? • Developmental surveillance is the routine monitoring and tracking of developmental milestones of all children at well-child visits to identify those at risk for any type of atypical development. • Screening refers to the use of standardized instruments applied to a population to identify those children at risk for a developmental disorder.
WHY ARE DEVELOPMENTAL SURVEILLANCE AND SCREENINGS IMPORTANT? • Many children with developmental disabilities miss the opportunity for early detection and intervention. • 17% of children have a developmental or behavioral disability. • Less that 50% of these children are identified as have a problem before starting to school. • Parents want and seek guidance from their personal care provider, but 65% of pediatricians feel inadequately trained children’s developmental status. • No national data tracking the use of developmental assessments and/or referral to early intervention services.
WHEN AND WHERE SHOULD SCREENINGS HAPPEN? Screening relies on being able to access parental participation. • Screening can occur at a time when other assessments are being done. • Screening should be an ongoing process and occur at regular intervals. • Screening can be provided when children visit a primary care or other medical provider to receive services such as immunization. • Screening can be done by other providers during routine visits or for the specific purpose of screening.
WHAT IS A DIAGNOSTIC EVALUATION? A diagnostic evaluation is a multifaceted process involving assessments, interviews, and observations. A comprehensive evaluation includes: • Review of relevant background information. • Parent/caregiver interview. • Child health history – prenatal and perinatal histories, past medical history. • Developmental and behavioral history.
Parental Barriers Identifiedin Early InterventionParent Survey and Focus Groups • Parents expressed appreciation for the services. • Concerns about how confusing it can be when accessing other services. • Lack of access to programs that have income eligibility criteria was the most significant barrier identified by parents. • Parents are facing catastrophic medial costs • Stress and constant demands result in a high divorce level among parents of children with disabilities.
Provider Concerns Identifiedin Early Intervention ProviderSurvey and Focus Groups Growing numbers of special needs children who are Hispanic and whose families do not speak English. • Teachers and Early Intervention providers were concerned because of the inability to communicate with the parents. • The providers are concerned with the lack of trained Hispanic early intervention professionals. • Fear that Hispanic families did not seek Early Intervention services for their special needs children due to fear of their illegal immigration status being identified.
Lack of Communication BetweenProviders A consistent comment by providers was that they didn’t communicate with each other. If a parent needed additional services, they didn’t feel confident that they were knowledgeable enough to refer them to available services.
Early InterventionStudy Recommendations • Promote the importance that all infants and young children should be screened for developmental delays. • Recommended screening schedule • Birth • 2, 4, 6, 9, 15, and 18 months • 2, 3, 4, 5, and 6 years of age. In Tulsa County, that would be: • approximately, 9,300 at birth • 55,800 screens in the first 2 years • 46,500 screens from age 2 years through 6 years of age • Screenings should address areas including: physical (fine and gross motor, vision, hearing), cognitive, communication (expressive and receptive), adaptive, social emotional.
Early InterventionStudy Recommendations • Educate the community • Collaboration • Develop a Data Tracking System. • Identify Capacity • Develop a Strategic Plan • Collaborate with the Hispanic Community