Download
1 / 22
220 likes | 327 Views
Addressing Central Changes in Patients with Chronic Low Back Pain . By Mo Sabri. Overview . Central changes in CLBP Advent of fMRI peripheral insult may not be to blame Gray matter density Chemical Cortical representation Manifestations of central changes

E N D
Addressing Central Changes in Patients with Chronic Low Back Pain By Mo Sabri
Overview • Central changes in CLBP • Advent of fMRI peripheral insult may not be to blame • Gray matter density • Chemical • Cortical representation • Manifestations of central changes • Decreased systemic pain tolerance • Motor impairments • Decreased capacity to make “emotional” decisions • Decreased body awareness • Building on evidence, I’ll make a few hypotheses as to how health care professionals can address the central symptoms to improve outcomes.
Chronic Back Pain is Common…And We Aren’t At Treating It Effectively! • Ten percent of adults suffer from severe chronic pain. (Apkarian 2004) • Back pain is the most common cause of activity limitation in people younger than 45 and the second most frequent reason for visits to the physician. (Grachev 2000) • LBP is the fifth most common reason for admissions to the hospital, and the third most common cause of surgical procedures. (Grachev 2000) • In 85% of doctors visits related to back pain, no definitive diagnosis can be made. (Apkarian 2004) • Not effectively treated pharmacologically in chronic state. (Grachev 2000)
Decreased Prefrontal and Thalamic Gray Matter in Patients with CLBP • Apkarian et al, 2004 • 26 pts with CLBP >6mo, 26 healthy controls • Used MRI and voxel-based morphometry to compare brain areas, cortical gray matter, etc. after normalizing for skull size. • Subjects filled out McGill pain questionnaire short form to derive data re: the sensory and affective dimensions of CBP.
Decreased Gray Matter (cont) Apkarian et al, 2004
Decreased Gray Matter (cont) • CBP pts displayed 5-11% less whole brain gray matter than healthy controls, the equivalent to that of 10-20 years of aging. • Longer pain duration is affiliated with greater gray matter loss. • Pts with neuropathic symptoms had slightly more degeneration than non-neuropathic patients. • The DLPFC and the Ant. Thalamus were the areas of the most degeneration • 14% less gray matter in non neuro patients • 27% less gray matter in pts with neuro symptoms • Duration of pain was the strongest predictor of degeneration (18%), followed by intensity, and affect. Apkarian et al, 2004
Cortical Changes= Chemical Changes • EgorGrachev et al, 2000 • Lumbosacralmalalignment is not enough to diagnose a patient with LBP- many asymptomatic people have positive MRI findings. • Used H-MRS to track different metabolites in the DLPFC, Cingulate cortex, and thalamus in 9 CBP patients, and 11 healthy volunteers. • DLPFC Chemical concentrations were 6.5% lower in CBP patients • Decreased: • glucose (marker of slowed cellular metabolism) • N-acetyl asparate see in in stroke, MS, Alzheimer’s, epilepsy • Increased pain and anxiety= more significant decreases
Somatosensory Cortex Changes in CLBP • Flor et al, 1997 • 10 pts with CBP and 9 age and gender matched controls • Patients were given painful and non painful estim second digit and back while magnetic fields from the contralateral hemisphere (over the somatosensory cortex) were recorded using biomagnetometer. Results: • Increased cortical response to the same stimuli (500μA) in patients who had increased chronicity of BP. • Cortical shift
Somatosensory Cortex Changes in CLBP (Cont) Representation of the back on the somatosensory cortex is expanded and shifted medially, where the leg is normally represented Flor et al 1997
What we’ve learned so far: • Apkarian, 2004- gray matter degeneration in CBP patients. • Longer duration>shorter duration of symptoms • Neuropathic>non neuropathic • Grachev, 2000- supports these findings with similar evidence related to decreased chemical concentrations • Decreased glucose and N-acetyl asparate in CBP pts • Flor, 1997- pain causes cortical representation to change • CBP pts have increased cortical response to stimuli • Medial shift and expanded representation of back in somatosensory cortex
Back pain + Brain changes= ? Manefestations of central changes: • Decreased systemic pain tolerance • Motor impairments • Decreased capacity to make “emotional” decisions • Decreased body awareness
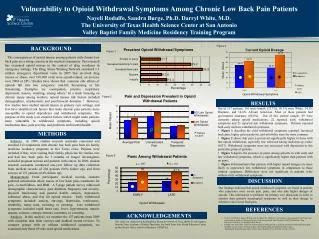
Decreased Systemic Pain Tolerance • CBP pts have a ↓ mechanical pain thresholds at lumbar spine, thumb, and other peripheral locations (Kobayashi 2009) • Hot noxious stimulation of the hand hurts more (Kleinbohl, 1999) • Pts with CLBP reported longer duration, higher intensity and more widespread pain after saline injection into the deltoid. (O’neill 2007) • Apkarian, 2006 noted that CLBP patients rated sour tastes as significantly more sour than their healthy counterparts.
Motor Impairments • Do cortical changes impair central drive? • Mehta et al, 2010 • 30 with CLBP (>3mo) and 30 controls • Trunk muscle activity of 4 groups of muscles: IO/TA, EO, RA, and “superficial lumbar multifidus”…? • 3 shoulder flexion trials in response to an auditory stimulus • Average pain intensity rating during the study was 4/10, and did not increase with the testing protocol.
Motor Impairments (cont) 0= onset of deltoid activation Caveat: this data looks good, but there is a wide distribution of data. Mehta et al, 2010
Decreased Capacity to Make “Emotional” decisions • Apkarian et al, 2004 investigated the emotional/behavioral aspects of CLBP • 26 CBP, 12 CRPS, 26 normal controls played the Iowa Gambling Task because it is thought to employ the DLPFC in decision making. • Results • CLBP and CRPS pts performed significantly worse on the gambling task • CLBP should be considered a “cognitive state” that competes with other cognitive abilities especially on tasks that use the same neural circuitry.
Decreased Body Awareness • Moseley et al, 2008 • Employed the CRPS paradigm to 6 CLBP pts and 10 healthy controls. • Draw the outline of your back as you feel it to be • Two point discrimination
WOAH! Who Knew Back Pain Was so complicated?! • Central changes • Gray matter degeneration • Chemical markers indicate degeneration • Cortical representation expands and shifts • Manifestations of central changes • Decreased systemic pain tolerance • Motor impairments- lose feed forward control • Decreased capacity to make “emotional” decisions • Decreased body awareness and two point discrimination
Does this mean that PTs should do more than Estim, heat, and ab strengthening for these people????????????
Let’s Borrow From Other Learning Paradigms! • Constraint induced movement therapy- we know cortical insult is not permanent. • Mehta (motor) • Moseley (body awareness) • Apkarian (decision making)