Download
1 / 38
380 likes | 506 Views
Chapter 13 Channels of Distribution. Norman V. Carroll, PhD Professor of Pharmacy Administration Virginia Commonwealth University School of Pharmacy Chapter 13 slides for Marketing for Pharmacists, 2nd edition. Learning Objectives.

E N D
Chapter 13Channels of Distribution Norman V. Carroll, PhD Professor of Pharmacy Administration Virginia Commonwealth University School of Pharmacy Chapter 13 slides for Marketing for Pharmacists, 2nd edition
Learning Objectives • Define and give examples of a channel of distribution for pharmacy products and services. • Define and give examples of members of channels of distribution for pharmacy products and services. • Define the term intermediary, give examples of intermediaries, and list and describe the functions intermediaries fulfill in channels of distribution.
Learning Objectives (continued) • Discuss the effects of customer, product, and manufacturer characteristics on channel structure and explain why different types of pharmacy products and services require different channel structures. • Define and give examples of channel conflict and cooperation. • List and explain the types of vertical marketing systems and discuss the need for them.
Learning Objectives (continued) • Explain the functions and services offered by pharmacy benefit managers and the effects these organizations have had on community pharmacy. • Explain how the growth of managed care has led to increasing cooperation and consolidation among pharmacy retailers and increasing conflict between retailers and other channel members.
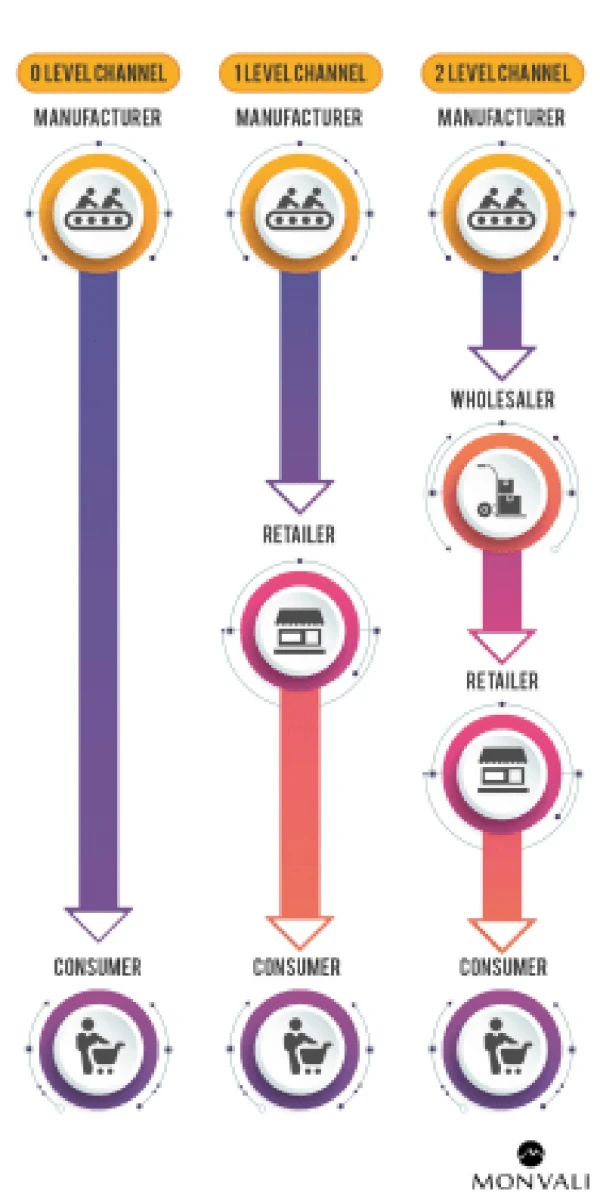
Traditional Channels MANUFACTURER WHOLESALER PHARMACY (Retailer) CONSUMER
Why have intermediaries? MANF RETAILER MANF RETAILER MANF RETAILER
Efficiency MANF RETAILER MANF RETAILER WHLSER MANF RETAILER
Additional functions of intermediaries • Product information - safe, effective use • Convenience - place and time • Variety / assortment • Services • Repackaging • Reimbursement • Repair • Credit
Traditional Channels MANUFACTURER WHOLESALER PHARMACY (Retailer) CONSUMER
Why long channels for pharmaceuticals? • Customer characteristics • Product characteristics • Manufacturer characteristics • Legal restrictions • What about new types of medicines?
Channel conflict - Discriminatory pricing - Limited distribution Channel cooperation - Buying groups - Prime vendors - Charge-back system
NO CHARGE-BACK MANUFACTURER AWP - 20% WHOLESALER AWP - 15% PHARMACY RETAIL
CHARGE-BACK SYSTEM MANUFACTURER AWP - 20% AWP x 25% WHOLESALER AWP - 40% HMO PHARMACY
Vertical Marketing Systems • Administered - based on power • Corporate - based on ownership • Contractual - license / franchise - wholesaler voluntary chains
MANF Merck WHOLESALER Cardinal RETAILER Medco / Medicine PAID Shoppe CONSUMER
PHYSICIANS Staff Model HMO HOSPITAL PHARMACY CONSUMER
Number of Community Pharmacies Source: IMS DDD Class of Trade Analysis
Managed Care Enrollment (000) Source: Managed Care Digest HMO-PPO Aventis MCD
3rd Party Payment for Rx Drugs IMS DDD Class of Trade Analysis
Sales of Mail Order Pharmacies Source: IMS DDD Class of Trade Analysis
PLAN SPONSOR Commonwealth of Virginia Medco PBM PHARMACY Rite Aid COVERED LIFE/BENEFICIARY D. Holdford
Why PBMs? • Growth of third-party payment • Increase efficiency of payment and information flows • Intermediary for payment and info
Plan Sponsors General Motors BCBS Aetna Teamsters Pharmacy Benefit Manager PBM Buford Rd. Pharmacy Wal-Mart Eckerd Rite Aid
PBM Services - early • Claims processing • Retail pharmacy network • Drug cards for beneficiaries • DUR and use management • Utilization reports to sponsors • Electronic processing • On-line adjudication
PBM Services - later - “managing the drug benefit” • Why – control drug costs • What – • Discount pharmacy reimbursement • Mail order – the three big PBMs each own one • Drug benefit design – co-pay, quantity limits, exclusions, three-tier designs • Formulary • Drug product rebates
What is a rebate? • Payment made by a manufacturer to a PBM or other entity that does NOT TAKE PHYSICAL POSSESSION OF THE DRUG • Usually on patented branded products • Based on use of the manufacturer’s drug • Given to encourage greater use • Substantial
Rebate Manf Goods Wholesaler PBM Payment Pharmacy Plan Sponsor Patient Rebates
PBM revenue sources • Administrative fees - per claim • Clear to sponsor, specified in contract • Competitive • Easy audit by sponsor • Services - like disease management • Relatively small revenues
PBM revenue sources • Rebates – old • Somewhat hidden from sponsor • Not clear in contract • Difficult for sponsor to audit • Mail order generics – new • Retail – MAC • Mail – AWP – 50% • For generics AWP-50% >> MAC
Effects of PBM rebates • PBM incentive - maximize rebates • Which products do they favor? • Low cost or high rebate? • Help consumer? • Help plan sponsor? • Pharmacists’ image?
Major Pharmacy Benefit Managers PBM Rx volume (millions) Caremark 432 Medco 397 Express 300 Total top-3 PBMs 1,129 Total retail rx volume 3,175
Major Pharmacy Benefit Managers PBM Owner Caremark McKesson (PCS) Lilly (PCS) Rite Aid (PCS) Advance Paradigm Advance/ PCS Baxter Indep Caremark PCS/Caremark CVS Caremark Medco IndependentMerck Independent Express Independent
Consolidation and Alliances • Corporate chains - Consolidation (horizontal integration) - Market power - Efficiency - Vertical integration - PBM • Voluntary chains (small chains and indeps) - Wholesalers - PBM functions
Consolidation in Chain Pharmacy 1990 1995 2005 Walgreens 1,525 2,085 4,962 Rite Aid 2,352 2,759 3,331 Thrifty 1,065 1,040 (Rite Aid) CVS 801 1,366 5,400 Revco 1,870 2,169 (CVS) Hook-SuperX 1,110 (Rev) (CVS) Eckerd 1,632 1,716 (CVS/ Coutu) Thrift Drug 472 640 (CVS/ Coutu) Jean Coutu 192 470 2,243 Totals 11,019 12,245 15,936
Wholesaler-Sponsored Voluntary Cooperatives Name Sponsor No. Pharmacies Health Mart McKesson 3,000 Valu-rite McKesson ? AccessHealth McKesson 3,000+ Family Pcys Amerisource- 2,500 Bergen (ABC) Good Neighbor ABC 2,500 Performance + ABC 3500+ Leader Cardinal 3,300
Retail Pharmacies - Efficiency • Higher-volume outlets • Economies of scale • Technology • Phone systems • Electronic links with prescribers • Robotics and automated dispensing • Centralized dispensing (fill) and adjudication • Web and phone-based refill services
Summary - Trends • Increasing third-party payment / managed care • Increasing mail order sales • Increasing importance of PBMs • Consolidation: • PBMs • Chain pharmacies • Sort of – community pharmacies • Increased efficiency