Download
1 / 30
300 likes | 422 Views
Heart. Special Pathology. The human heart is a remarkably efficient, durable, and reliable pump; propels over 6000 liters of blood through the body daily beats more than 40 million times a year during an individual's lifetime, thereby

E N D
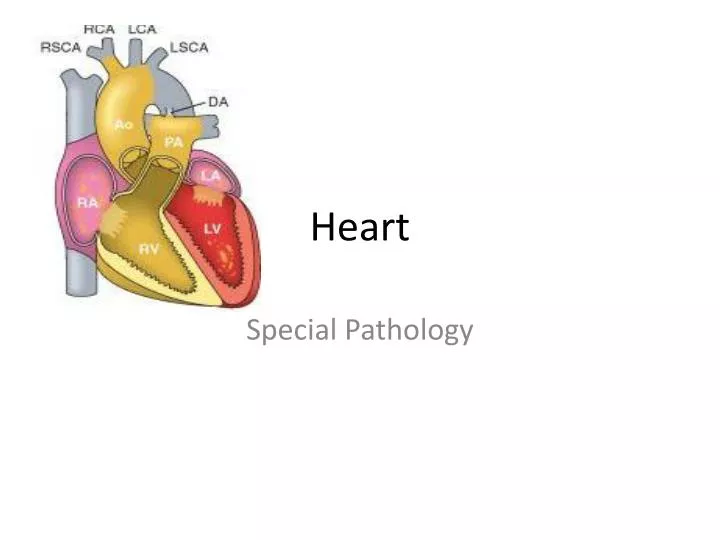
Heart Special Pathology
The human heart is a remarkably efficient, durable, and reliable pump; • propels over 6000 liters of blood through the body daily • beats more than 40 million times a year during an individual's lifetime, thereby • providing the tissues with a steady supply of vital nutrients and • facilitating the excretion of waste products.
The normal heart weight varies with body height and weight; • 250 to 300 g in females • 300 to 350 g in males. • The usual thickness of the free wall of; • right ventricle is 0.3 to 0.5 cm • left ventricle 1.3 to 1.5 cm • increases in cardiac size and weight accompany many forms of heart disease. • Greater heart weight or ventricular thickness indicates hypertrophy, • enlarged chamber size implies dilation. • An increase in cardiac weight or size (owing to hypertrophy and/or dilation) is termed cardiomegaly.
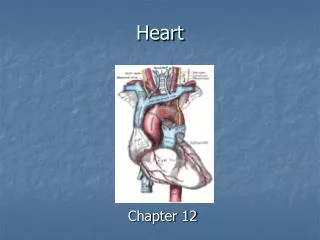
Cardiac myocytes • Basic to the heart's function is the near-inexhaustible cardiac muscle, the myocardium, • composed primarily of a collection of specialized muscle cells (Fig.). • They are arranged largely in a circumferential and spiral orientation around the left ventricle • chamber that pumps blood to the systemic circulation • Cardiac myocytes have five major components: • (1) cell membrane (sarcolemma) and T-tubules, for impulse conduction; • (2) sarcoplasmic reticulum, a calcium reservoir needed for contraction; • (3) contractile elements; • (4) mitochondria; and • (5) nucleus • Cardiac muscle cells contain many more mitochondria between myofibrils than do skeletal muscle cells • (approximately 23% of cell volume vs. 2%), • almost complete dependence of cardiac muscle on aerobic metabolism • Cardiac muscle cells each usually contain one spindle-shaped nucleus • Ventricular muscle contracts during systole and relaxes during diastole
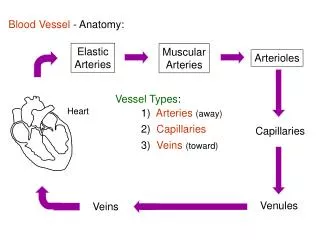
Three major epicardial coronary arteries; • (1) right coronary artery (RCA) • (2) left anterior descending (LAD) • (3) left circumflex (LCX) arteries, • both arising from left (main) coronary artery, • Branches of the LAD • diagonal and septal perforators • Branches of the LCX • obtuse marginals • Most coronary arterial blood flow to the myocardium occurs during ventricular diastole, • microcirculation is not compressed by the cardiac contraction
The right and left coronary arteries function; • End arteries • Although anatomically most hearts have numerous intercoronary anastomoses (collateral circulation) • Little blood courses through these channels in the normal heart • When one artery is severely narrowed, • blood flows via collaterals from the high to the low pressure system • causes the channels to enlarge • Progressive dilation of collaterals; • stimulated by ischemia, • play a role in providing blood flow to areas of the myocardium otherwise deprived of adequate perfusion • When the principal blood flow is compromised and collateral blood flow is inadequate, • subendocardium (myocardium adjacent to the ventricular cavities) • area most susceptible to ischemic damage
Aging • knowledge of changes in the cardiovascular system that are expected to occur with aging is important; • With an increasing number of persons surviving into their eighth decade and beyond, • number of individuals aged 65 years and older will approximately double from 2000 to 2050 • (from 35 million to 79 million in the United States) • Changes associated with aging occur in; • pericardium, • cardiac chambers, • valves, • epicardial coronary arteries, • conduction system, • myocardium, • aorta
With advancing age; • amount of epicardial fat increases, • particularly over the anterior surface of the right ventricle and in the atrial septum. • A reduction in the size of the left ventricular cavity; • particularly in the base-to-apex dimension, accentuated by systemic hypertension • sigmoid septum • rightward shift and tortuosity of a dilated ascending aorta, this chamber alteration causes the basal ventricular septum to bend leftward, bulging into the left ventricular outflow tract • Such reduction in the size of the left ventricular cavity can simulate the obstruction to blood leaving the left ventricle • often occurs with hypertrophic cardiomyopathy
Several changes of the valves; • Calcification of the mitral annulus and aortic valve, the latter frequently leading to aortic stenosis • Valves can develop fibrous thickening, • mitral leaflets tend to buckle back toward the left atrium during ventricular systole, • simulating a prolapsing (myxomatous) mitral valve • Many older persons develop small filiform processes (Lambl excrescences) ; • closure lines of aortic and mitral valves; • arising from the organization of small thrombi on the valve contact margins
Compared with younger myocardium, "elderly" myocardium also has; • fewer myocytes, increased collagenized connective tissue and, in some individuals, deposition of amyloid • In the muscle cells, lipofuscin deposits, and basophilic degeneration, an accumulation within cardiac myocytes of a gray-blue byproduct of glycogen metabolism, may be present. • Extensive lipofuscin deposition in a small, atrophied heart is called brown atrophy; • often accompanies cachectic weight loss, as seen in terminal cancer. Although the • morphologic changes described are common in elderly patients at necropsy, and they may mimic disease, • Only in a minority are they associated with clinical cardiac dysfunction.
Cardiac pathology • Although many diseases can involve the heart and blood vessels, • cardiovascular dysfunction results from one or more of five principal mechanisms: • Failure of pump • Obstruction to flow • Regurgitant flow • Disorders of cardiac conduction • Disruption of the continuity of the circulatory system
Failure of the pump; • cardiac muscle contracts weakly or inadequately, and the chambers cannot empty properly • In some conditions, however, the muscle cannot relax sufficiently to permit ventricular filling • Obstruction to flow; • owing to a lesion preventing valve opening or otherwise causing increased ventricular chamber pressure (e.g., aortic valvular stenosis, systemic hypertension, or aortic coarctation). • The increased pressure overworks the chamber that pumps against the obstruction.
Regurgitant flow; • causes some of the output from each contraction to flow backward, • adding a volume workload to each of the chambers, which must pump the extra blood • (e.g., left ventricle in aortic regurgitation; left atrium and left ventricle in mitral regurgitation). • Disorders of cardiac conduction; • Heart block or arrhythmias owing to uncoordinated generation of impulses • (e.g., atrial or ventricular fibrillation) • lead to nonuniform and inefficient contractions of the muscular walls. • Disruption of the continuity of the circulatory system; • permits blood to escape • (e.g., gunshot wound through the thoracic aorta).
The major categories of cardiac diseases • congenital heart abnormalities, • ischemic heart disease, • heart disease caused by systemic hypertension, • heart disease caused by pulmonary diseases (corpulmonale) • diseases of the cardiac valves, • primary myocardial diseases
Manifestations of Cardiac Diseases; • Pain • Ischemic Pain • Pericardial Pain • Cardiac Enlargement • Hypertrophy • Dilatation • Abnormal Cardiac Rhythm • Arrhythmia • Dysrhythmia
Ischemic Pain; • The most common cause of cardiac pain is myocardial ischemia • caused by stimulation of nerve endings by the lactic acid produced during anaerobic glycolysis • classically is retrosternal • usually described as constricting in nature • may radiate to the back, to either arm (especially the left), or up the neck into the jaw. Pain varies in severity from mild to excruciating • Angina pectoris; • ischemic pain • induced by exercise sometimes by stress or cold • relieved by rest. • Pericardial Pain; • Inflammation of the parietal pericardium • sharp lower retrosternal pain • vary with posture and respiration. It is often • accompanied by signs of pericardial inflammation • pericardial rub and effusion.
Cardiac Enlargement; • Dilation of the cardiac chambers • heart failure, myocarditis • hypertrophy of the walls • hypertension, many valvular defects • Cardiac dilation and hypertrophy do not cause clinical symptoms • useful indications of the presence of cardiac disease • recognized by clinical examination, radiography, or electrocardiography • Documentation of cardiac hypertrophy at autopsy is usually done by measuring the thickness of the walls • Right ventricle thickness exceeding 0.5 cm - RVH • left ventricular thickness exceeding 1.5 cm - LVH
Abnormal Cardiac Rhythm; • Arrhythmia; Dysrhythmia • Normal cardiac contraction; • Sinoatrial (SA) – initiate the impulse in right atrium • Atrioventricular (AV) node – conduct impulse from atria to ventricles • His-Purkinje system - Spread impulse in the ventricular mass • Ventricular contractions are coordinated by the branches of the AV node. • Arrhythmias reflect; • (1) altered activity of the SA node, • (2) the development of "new" ectopic foci that drive the heart at an accelerated or irregular rate, • (3) conduction defects
Methods of Evaluating Cardiac Structure & Function; • Physical Examination • Arterial Pulse • Jugular Venous Pulse • Cardiac Apex Beat • Auscultation of the Heart • Electrocardiography • Imaging studies • Cardiac Catheterization • Endomyocardial Biopsy
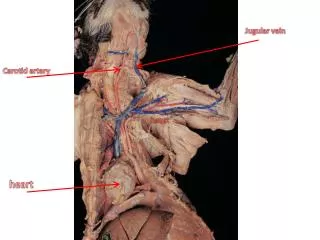
Arterial Pulse; • Palpation of the carotid and radial artery pulses permits recognition of; • rate and rhythm of ventricular contraction • subtle changes in the pressure wave associated with certain cardiac diseases; • sustained low-volume pulse in aortic valve stenosis • bounding pulse in aortic valve incompetence
Jugular Venous Pulse; • The height of the internal jugular vein pulse wave • clinical estimate of central venous pressure • increased in right heart failure, volume overload, and pericardial tamponade or constriction • Alteration of the wave form of the jugular venous pulse also provides important information • accentuation of the first, or a wave indicates that the pressure in the right side of the heart is increased • absence of the a wave is a sign of atrial fibrillation
Cardiac Apex Beat; • Localization of the cardiac apex beat by palpation • rough evaluation of cardiac enlargement • A sustained heave at the apex is characteristic of left ventricular hypertrophy; • a heave at the left parasternal border occurs with right ventricular hypertrophy
Auscultation of the Heart • Normal heart usually has two sounds; • first due to closure of the atrioventricular valves • second due to closure of the semilunar valves ( • usually perceived as slightly split because of asynchronous closure of pulmonary and aortic valves • Various additional sounds may signify disease • third heart sound (triple, or gallop, rhythm) may occur as a result of rapid ventricular filling in diastole and is seen in heart failure and mitral incompetence. • An opening snap suggests; • mitral stenosis; a fourth heart sound, pulmonary or systemic hypertension; and a friction rub, pericarditis. • Cardiac murmurs; • turbulence of blood flow through the heart, • usually across damaged valves and abnormal pressure gradients • Soft, innocent ejection systolic murmurs occur in high-output states • fever or anemia and during vigorous exercise • Murmurs signifying congenital and valvular heart disease
Electrocardiography • Graphic display of the electrical activity of the heart as recorded on the body surface by appropriately placed electrodes. • Normal electrocardiographic tracing can be divided into; • (1) the P wave, due to atrial depolarization; • (2) the PR interval, which is a rough measure of conduction time through the atrioventricular node; • (3) the QRS complex, due to ventricular depolarization; and • (4) the T wave, due to ventricular repolarization. The ST segment is isoelectric (ie, level with the baseline) in the normal physiologic state. • The ECG provides valuable information for assessment of • (1) cardiac hypertrophy, • (2) arrhythmias and conduction delays, • (3) myocardial ischemia and infarction, • (4) pericardial disease, • (5) electrolyte abnormalities (especially K+, Mg2+, Ca2+) and some drug effects (eg, digitalis).
Imaging studies • Echocardiography; • (M-mode, two-dimensional, Doppler, stress, and transesophageal) • means of evaluation of cardiac structure with sound waves reflected from the heart • Chest radiography; • gross cardiac structure and size • Magnetic resonance imaging (MRI), radionuclide imaging, cine-computed tomography (CT), and positron emission tomography (PET) • newer modalities.
Cardiac Catheterization • insertion of a catheter through; • a vein - right heart • an artery - to the left heart • evaluation of pressures and oxygen saturation in the various chambers • angiography • Injection of radiopaque dye • visualization and photography of the contracting heart and the coronary arteries.
Endomyocardial Biopsy; • Tissue can be taken from the inner surface of the heart with a biopsy forceps passed in a manner similar to a cardiac catheter. • The main indications for endomyocardial biopsy are diagnosis of suspected; • myocarditis • cardiomyopathy • organ rejection after heart transplantation