Download
1 / 314
3.15k likes | 3.36k Views
HEART. By Mary Yvonnette C. Nerves, MD, FPSP. Once I had brains, and a heart also; so having tried them both, I should much rather have a heart. --The Tin Woodsman of Oz. NORMAL. NORMAL. Weight: 250 to 300 g in females 300 to 350 g in males Thickness of the free wall:

E N D
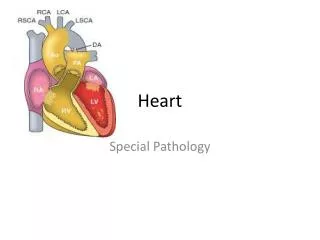
HEART By Mary Yvonnette C. Nerves, MD, FPSP
Once I had brains, and a heart also; so having tried them both, I should much rather have a heart. --The Tin Woodsman of Oz
NORMAL • Weight: 250 to 300 g in females 300 to 350 g in males • Thickness of the free wall: RV = 0.3 to 0.5 cm. LV = 1.3 to 1.5 cm.
Hypertrophy: greater heart weight or ventricular thickness • Dilation: an enlarged chamber size • Cardiomegaly: an increase in cardiac weight or size (owing to hypertrophy and/or dilation)
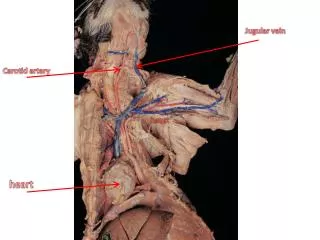
Layers of the heart: • Epicardium • Myocardium • Endocardium Pericardium: fibrous covering around the heart
Myocardium • composed primarily of a collection of specialized muscle cells calledcardiac myocytes • Ventricular muscle contracts during systoleand relaxes during diastole • Sarcomere: functional intracellular contractile unit of cardiac muscle
BLOOD SUPPLY • (3) Major Epicardial Coronary arteries: a. Left Anterior Descending Artery - Anterior wall - Anterior two thirds of septum - Entire apex of heart, circumferentially b. Left Circumflex Coronary Artery - posterior, lateral left aspect of heart. c. Right Coronary Artery - posterior one third of septum, inferior aspect, and posterior wall of heart.
VALVES 1. Semilunar valves a. Aortic valve b. Pulmonary valve 2. Atrioventricular valves a. Mitral valve b. Tricuspid valve
PATHOLOGY • Failure of the pump • An obstruction to flow • Regurgitant flow • Disorders of cardiac conduction. • Disruption of the continuity of the circulatory system
Congestive Heart Failure (CHF) • pathophysiologic state resulting from impaired cardiac function that renders the heart muscle unable to maintain an output sufficient for the metabolic requirements of the tissues & organs of the body
Congestive Heart Failure (CHF) • the physiology of HF involves an interplay between 2 factors: a) inability of the failing heart to maintain sufficient cardiac output to support body functions b) recruitment of compensatory mechanisms to maintain cardiac reserve
Cardiac output: amt of blood that the heart pumps each minute - reflects how often the heart beats each minute (HR) and how much blood the heart pumps with each beat (SV) CO = HR x SV
Causes of CHF • Pump Failure: Failure that is intrinsic to the myocardium. • Two types: • Systolic Failure: Failure to pump blood out of heart. • Diastolic Failure: Failure to distend the heart to fill the ventricles, as in constrictive pericarditis. • Most common reason for pump failure is from myocardial hypertrophy, usually sec. to HPN.
Conduction System Failure: Secondary to MI • Valvular Failure: Inflammatory (endocarditis), autoimmune, or congenital. • Cardiac Malformations: Congenital • Blood Loss / Obstruction of Blood Flow: Extracardiac causes. Pulmonary emboli or bleeding.
Mechanisms that maintain arterial pressure and perfusion of vital organs in the presence of excessive hemodynamic burden or disturbance in myocardial contractility: • Frank-Starling mechanism - increased preload of dilation helps to sustain cardiac performance by enhancing contractility • Myocardial structural changes - augmented muscle mass w/ or w/o cardiac chamber dilation, in which the mass of contractile tissue is augmented
Activation of neurohumoral systems • release of the neurotransmitter norepinephrine by adrenergic cardiac nerves • activation of the renin-angiotensin-aldosterone system, and • release of atrial natriuretic peptide.
Heart’s compensatory changes • Hypertrophy • Ventricular dilatation • Blood volume expansion by salt & water retention • Tachycardia
Extent of hypertrophy varies for different underlying causes: • 350 – 600 gms: pulmonary HPN / IHD • 400 – 800 gms: systemic HPN / aortic stenosis / mitral regurgitation / dilated cardiomyopathy • 600- 1000 gms: aortic regurgitation / hypertrophic cardiomyopathy
The pattern of hypertrophy reflects the nature of the stimulus: 1. Pressure-overload (concentric) hypertrophy • Pressure-overloaded ventricles (e.g., in hypertension or aortic stenosis) develop pressure-overloadhypertrophy of the LV, with an increased wall thickness • LV: the augmented muscle may reduce the cavity diameter • the predominant deposition of sarcomeres is parallel to the long axes of cells; cross-sectional area of myocytes is expanded (but cell length is not).
2. Volume-overload hypertrophy • volume overload stimulates deposition of new sarcomeres and cell length (as well as width) is increased • characterized by dilation with increased ventricular diameter • muscle mass and wall thickness are increased approximately in proportion to chamber diameter
Left-sided CHF • Failure of the left side of the heart to pump sufficient blood • Common causes of left-sided failure • Ischemia (old or recent myocardial infarct, ischemic muscle disease) • Aortic or mitral valve disease • Systemic hypertension • Myocardial disease / cardiomyopathy
Clinical manifestations: • Pulmonary congestion and edema • Reduced cardiac output also causes reduced renal perfusion, leading to • Further salt & water retention • Ischemic acute tubular necrosis • Impairment of waste excretion, causing prerenal azotemia • CNS perfusion is reduced, often resulting to hypoxic encephalopathy
Right-sided CHF • Failure of the right side of the heart to pump enough blood • Common causes of right-sided failure • Pulmonary emboli (acute or chronic) • Any disease interfering with lung ventilation Emphysema / Cystic fibrosis • Left-sided heart failure! • Cardiac defects with left-to-right shunts
Clinical manifestations: • Portal, systemic and dependent peripheral congestion & edema & effusions (pleural & peritoneal) • Hepatomegaly w/ centrilobular congestion & atrophy of central hepatocytes nutmeg liver (chronic passive congestion) • Centrilobular necrosis • Cardiac sclerosis • Congestive splenomegaly • Renal congestion
HEART DISEASE • Congenital heart disease • Ischemic heart disease • Hypertensive heart disease (systemic & pulmonary) • Valvular heart disease • Nonischemic (primary) myocardial disease • Cardiac Neoplasms
CONGENITAL HEART DISEASE • Abnormalities of the heart and great vessels present at birth • Most common type of heart disease among chldren • Occurs during 3rd to 8th week of gestation • Incidence: 1% of livebirths • Higher incidence among prematures and stillborn
Origin of the Heart Angioblasts Angioblasts (heart forming cells) first appear at 18 days Two dorsal aortae develop and subsequently fuse in the mid-line to form a primitive heart tube. Heart first forms rostral to the neural plate As the brain grows, the heart moves caudally into the neck and then into the chest 18 days Heart 22 days Heart Late presomite embryo Heart at 18 to 22 days