Download
1 / 25
300 likes | 350 Views
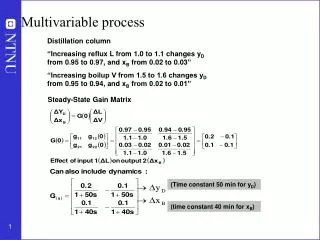
PHOTODYNAMIC THERAPY: an attractive but complex multivariable process. A. Illanes, Ph.D. Outline. Introduction to PDT The PDT process Main Variables Some applications in oncology Limitations of PDT Important dynamical information of the process System identification vision.

E N D
PHOTODYNAMIC THERAPY: an attractive but complex multivariable process A. Illanes, Ph.D
Outline • Introduction to PDT • The PDT process • Main Variables • Some applications in oncology • Limitations of PDT • Important dynamical information of the process • System identification vision
Introduction: What is Photodynamic Therapy (PDT) Photochemical reaction involving: Main objective: Photosensitizer (PS) Light O2 Generation of ROS 3 main components • highly cytotoxic reactive oxygen species 3 pathways of cell damage
Introduction: main steps of the PDT process Therapy Transportation of PS inside the tumor Waiting time Photosesitizer Excited state Tissue O2 exogeneously endogeneously light singletO2 Injecting PS ALA (better tumor selectivity) Photosesitizer Ground state Celullar toxicity (ROS) ALA application Beginning of therapy time
Photosensitizer Fakir-PDT Usually for thicker (>2cm) and deeper tumors (>2mm) systemic Topical Systemic Interstitial SUMINISTRATION Dermaroller/Stamp • Critical factors of PS for PDT effectiveness: • Distribution of PS in tissue • Delivery and transportation of PS • Ideal characteristics of PS: • It should have a high absorption peak between 600-800 nm • High photostability low photobleaching • high rate of ROS generation • Good pharmacokinetics properties • Large degree of selectivity • Accumulation in tumor compared to normal tissue ALA Mixture
Light delivery critical factors Single Fractionated – hyper Fractionated Metronomic Light delivery mode Fluorescence excitation Action spectra Choice of access of light Light distribution Light wavelength As much homogeneous as possible
Oxygen murine tumor example Perfusion Hypoxia • Critical factors of O2 for successful PDT outcome: • Tumor O2 concentration • O2 depletion produces by reaction • Requirement of a sufficiently large concentration of O2 in the tumor tissue (Photofrin, 5 mg/kg, 75 mW/ cm2, 135 J/cm2) 30 minutes of PDT No ROS generation During irradiation O2 O2 depletion PDT IS CAPABLE OF INDUCING HYPOXIA WHICH CAN LIMIT THE EXTENT IN PDT DAMAGE • Due to rapid consumption of O2
Some important remarks • Dermatology • Skin cancers located mainly in the head and neck areas (80%) • Golden standard for treatment is surgical tumor excision • PDT has shown excellent cosmetic outcomes • Skin cancer is very attractive for PDT in terms of PS delivery (topically) • Easy access for PS • Less time interval between PS delivery and light administration • However … less light penetration • Other tumors (esophagus, bladder, prostate) • PS delivery very complicate only systemic • Light delivery good penetration • Not stratum corneum • Very good penetration in mucosal areas • Geometry can be a problem for light homogeneity
Barriers of adoption into routine clinical practices • More than 250 randomized clinical trials have been officially reported • essentially all types of solid tumors with the exception of melanotic melanoma have been found to be positively responsive to PDT • However treatment relatively slow to enter mainstream in clinical practice • PDT can be considered a reasonable option for some applications • However, its effectiveness in the management of other types of tumors has not yet been unequivocally proven. • The major reasons: • only a few adequately powered randomized controlled trials have been performed to date • lack of optimal PDT parameters (illumination conditions, PS dose, monitoring)
Main limitations of PDT • Ineffective against metastatic lesions highly localized nature of PDT • Complexity of the process and the interrelationship of the involved variables … not a complete understood process • Pain during some treatment protocols • PDT produces mostly superficial effects. • Still about 1 in 4 or 5 patients ultimately does not respond to the treatment and it is not understood why particular patients fail to respond Problem: the deeper the tumor (and the thicker the cornea) the less ALA and light arrives
Many questions about the process What kind of patient (skin type, age), and tumorentity (AK, BCC, SCC,metastasis) needs what kind of photosensitizer (5-ALA. esther) in which pharmaceutical formulation (galenics) and how much activated PPIX/mm2 in what wave length (blue, greeen, red), light dosis and intensity to be curative treatable?
Time constants and values involved in PDT process • Time between PS administration and light exposure • > 24 hours systemic (dark room wait time) • > 3 hours topical • Maybe less using nano-emulsion • Light exposure time: 5 minutes – 3 hours • depending on modality • Time interval between PDT sessions: hours, daily, weekly • Size of solid tumors that would be interesting to treat: 1-10 cm (depth > 1mm) • Lifetime of generated ROS 30 – 180 ns (10 – 320 ns in some works) • Photodynamic damage occurs very close to PS location (10 – 55 nm)
Time constants and values involved in PDT process • Wavelength used for fluorescence and therapy • PPIX Fluorescence: Excitation 405 nm (380-440 nm), emission spectrum 635 nm (also 700-710 nm) • Therapy: 635 +- 5 nm • Photon intensity for producing ROS: • In principle the production of ROS requires an energy of 22.5 kcal/mole • Light up to only 800 nm can generate ROS longer WL have insufficient energy for generating PDT reaction • Time and values of different light delivery modes: seconds-minutes 20-50 mW/c^m2 20-150 mW/c^m2 hours 20-50 mW/c^m2 Hours - daily < 10 mW/c^m2
Time constants and values involved in PDT process • PPIX spectral dynamical changes Given the time constant involved in the process • Necessity of constant monitoring of variables for dosification • Given • Localized effect of PDT reaction • Variation of PS in tumor • Size and depth of solid tumor • Distributed measurements • Therapy of the whole tumor
Important variables and parameters in PDT • PS • PS availability (PPIX) • Oxygen • Tumor O2 concentration • Light source • fluence rate (mW/cm2) • Total light fluence (J/cm2) • Irradiation duration • Total light dosis • Tumor • Size • depth of tumor • Location • accessibility Dynamic and time-variant characteristics of many of these quantities ALA Waiting time Therapy Monitoring Dosimetry? still PS? When to start?
Monitoring • Blood flow • Correlation between DRS’s measured at different time instants • diffuse correlation spectroscopy (DCS) • Oxygen • Changes of light absorption and scattering in tissue • diffuse reflectance spectroscopy (DRS) • diffuse optical tomography (DOT) • spatial frequency domain imaging (SFDI) • PS • Fluorescence spectra • Photobleaching of PPIX • ROS detection • Light source • Isotropic probe
Challenges of Monitoring: system identification vision • Very Complex process • How to identify the process • through which observations • Obtained In a reduced space • Of difficult accesibility • In real time Time/space variant process For valuable quantitative information feedback Dosimetry
System identification vision Parametrical dynamical model (reduced model to some important dynamics) Signal processing Featture extraction Dosimetry model Observation of the process Monitoring PDT Process Treatment strategy
Conclusions • PDT has not yet been introduced in clinical practice for tumor therapy • Main problem: complex and still hardly understood dynamical relationship between the involved variables • Process difficult to monitor and optimize • Dosimetry and drug-light interval are crucial issues of the process • necessity of online monitoring • Process strongly time and space variant • Need of signal processing and system identification approaches
System identification vision: a example • PDT could be an effective and minimally invasively applicable way to treat many different types of tumors • without radiation and large incisions by just applying a light pulse • it is unclear when the most appropriate timing for this light pulse after ALA injection is. Open question • Drug-light interval can be predicted using system identification methods • Observations: fluorescence of the recursors instead of the one of the PS
System identification vision: an example Observations Dynamical model Identifiability??? PPIX prediction