Download
1 / 30
300 likes | 302 Views
This overview discusses the rationale, clinical evidence, and considerations for future studies regarding the use of preemptive or supportive renal replacement therapy (PCRRT/CVVH) before established renal failure in septic shock. It explores the history and advancements of CRRT, the pathophysiology of sepsis, and the potential benefits and risks of early initiation of CRRT.

E N D
Renal supportive therapy in septic shock Any evidence for preemptive or supportive use of PCRRT/CVVH before established renal failure ? Joachim E. Fischer, MD MSc University Children’s Hospital & Center for Integrative Human Physiology University of Zurich Eidgenössische Technische Hochschule Zürich Swiss Federal Institute of Technology Zurich
Overview • Rationale & Epidemiology • Clinical evidence • Other examples of technological advances • A word of caution • Consideration for future studies
The history of CRRT 1977 Kramer et al: CAVH 1986 Ronco et al: case series of four neonates 1990s Advances in machinery 40% of ICUs use CRRT 30% peritoneal dialysis 20% conventional hemodialysis 2000s Most PICU have CRRT available Indications: severe oliguria or anuria metabolic acidosis, ph < 7.1 hyperkalemia, > 6.5 mmol/l azotemia, urea > 30 mmol/l
Sepsis, adult patients • US: 700‘000 cases per year • US: 210‘000 deaths per year • US: Mortality > myocardial infarction • Renal failure + sepsis: mortality 70% • Renal failur alone: mortality 45% • Lower mortality in pediatric patients
Pathophysiology I • Untreated sepsis rapidly progresses from sepsis to severe sepsis, septic shock and multiple organ failure. • Sepsis is the organisms response which increases the chance of bacteria elimination at the risk of loosing control of the balance between inflammatory and anti-inflammatory responses
Sepsis cascade • Vasodilatation • Distributive shock N Engl J Med 2004;351:159-69
Treatment NEJM 2001:345:1368-77
Renal failure N Engl J Med 2004;351:159-69
Renal failure II • Supportive Interventions may prevent acute renal failure N Engl J Med 2004;351:159-69
Any help from CRRT? • Therapeutic efficacy in renal failure? • What is the best method?
Replacement in adult sepsis with renal failure N Engl J Med 2002;347:895-902
Rationale for CRRT in non-renal failure • Evolution did not plan for antibiotics, fluid resuscitation and ventilators • With advent of early aggressive therapy no biological need for inflammatory escalation • However: risk of fluid overloadin failing kidney • CRRT as supportive therapy similar to: • Ventilation (respiratory support) • Catecholamines and inotropic support
What is established? • ppCRRT registry group • Prospective observational collaboration • First report on 157 patients in 2005 • Data suggest fluid load as risk factor in pediatric patients with MODS • Data suggest goal directed fluid management in children
The tempting perspective • No one waits with ventilation until respiratory arrest • One does not withold catecholamines until circulatory arrest • CRRT may remove deleterious water soluble factors from blood Why postpone CRRT until renal failure ?
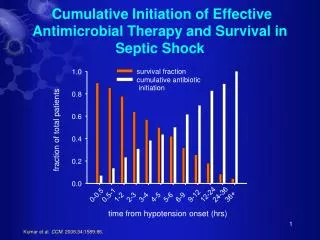
CRRT Approaches • Peak concentration hypothesis • Ronco et al: „The nonselective control of the peaks of inflammation and immunoparalysis may contribute to bring the patient to a lesser degree of imbalance…“ (Artif. Organs 2003; 27:792-801) • Importance of early initiation and appropriate UF rate (35 ml/kg/h)(Ronco et al. Lancet 2001; 356: 26-30)
Open questions • The optimum indication to initiate CRRT • Appropriate technique • Appropriate duration • Benefit / harm ratio differential across varous patient groups • Newborns • Iatrogenic sepsis after surgery • Severe comorbidities • Sepsis in immuncompromized patients
The history of pulmonary artery catheters • 1970s: First publications • 1980s: Clinicians consider it unethical to withhold catheter in critically ill • 1990s: Doubts whether additional clinical data alter outcome • 2000s: Multicenter RCT fail to show benefit, higher rate of pulmonary embolism
Example II: Drugs in sepsis • Experimental data suggested benefit of: • TNF-antibody • GCSF • Multicenter randomized controlled trials: • No benefit or adverse outcomes
The life-saving drug: Drotregocin ? N Engl J Med 2001;344:699-709
Multicenter RCT in septic shock N Engl J Med 2001;344:699-709
Drtotregocin revisited: no advantage survival N Engl J Med 2005;353:1332-41.
Drtotregocin revisited: more complications N Engl J Med 2005;353:1332-41.
A word of caution • Critical care is full of examples in which experimental evidence was favourable and clinical benefit was simply assumed. • Therapies that assist survival in the sickest patients may not prove to conver any advantage in medium to low risk patients
Future for CRRT in pediatric sepsis patients • Preemptive CRRT may be beneficial • CRRT is associated with increased risk of short-term and long term complications • Currently, ambiguity as to the possible benefits or harms of preemptive CRRT • It is likely that the benefit / harm ratio may differ amongst patients
Suggested approach to CRRT in sepsis • Currently, there is a lack of sufficient evidence to support the routine preemptive use of CRRT in pediatric patients with sepsis. • Given the potential harm it may be unethical to apply preemptive CRRT in pediatric sepsis patients outside the context of clinical studies • The ppCRRT registry group may provide the ideal platform for starting appropriate trials
Suggested approach II • Design of multi-center protocol of large randomized controlled trials to identify: • Optimal inclusion criteria: • Plasma compound threshold • Intervention threshold • Physiological measures threshold • Time of enrolment during the course of sepsis • Duration of supportive therapy • Comparison with other intervention strategies