Download
1 / 72
720 likes | 890 Views
The New Survey Process Quality Indicator Survey (QIS). Presented by: Janet McKee, MS, RD, LD President of Nutritious Lifestyles, Inc. QIS DEVELOPMENT. University of Colorado, University of Wisconsin, Maverick Systems, and Alpine Technology Development from 1998-2005

E N D
The New Survey ProcessQuality Indicator Survey(QIS) Presented by: Janet McKee, MS, RD, LD President of Nutritious Lifestyles, Inc.
QIS DEVELOPMENT • University of Colorado, University of Wisconsin, Maverick Systems, and Alpine Technology • Development from 1998-2005 • Field tests by research, CMS staff, CO, IA, MD, NJ and WI • Demonstration and evaluation by CA, CT, KS, LA, OH 2006
QIS DEVELOPMENT • New survey process started in Florida in November, 2006 • Florida statewide rollout- 2007 • Northern Florida first with migration to South
QIS PURPOSE AND OBJECTIVES • To guide surveyors through the federal survey process • Improve consistency and accuracy of Quality of Care/Quality of Life problem identification using a more structured process • Comprehensive review of regulatory care areas using current resources
QIS PURPOSE AND OBJECTIVES - continued • Enhanced documentation by organizing survey findings through automation • Focus survey resources on facilities with largest number of quality concerns • For providers, makes IDR process more difficult
QIS SURVEYTwo-stage computer-assisted survey process, which includes 9 Tasks
Good NewsThe survey process has changed, but the F-Tags and Interpretive Guidelines are the same.
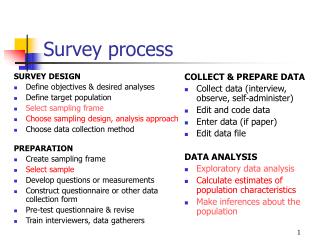
STAGE I PROCESS • Preliminary investigation of residents • Randomly selected by QIS Data Collection Tool (DCT) • Based on a range of care areas covered by the federal regulations • Resident assessments are based on observations, interviews, and review of the clinical records
STAGE I PROCESS – continued • The computer selects the residents using the MDS data • Constructs 160 resident outcome and process indicators called Quality of Care Indicators (QCIs) • The computer analyzes the on-site collected data
STAGE I PROCESS - continued • The QCIs are then compared to national norms • QCIs that score above the statistical threshold are computer-selected for a detailed in-depth investigation in stage II. • Includes Tasks 1-6 • QIS Manualhttp://ahca.myflorida.com/MCHQ/Long_Term_Care/LTC/index.shtml
STAGE II PROCESS • In-depth investigation of residents with care areas identified by the computer in Stage I that exceeded thresholds (national norms) • Triggered care areas and residents are systemically investigated using Critical Element Pathways to determine regulatory compliance • Includes Tasks 6-9
TASK 1: OFF-SITE SURVEY PREPARATION • Review OSCAR 3 report to determine if facility has a history of repeat deficiencies. • Review complaints filed with the agency in order to facilitate investigation during the survey. • Team assignments: census reconciliation, tour, and facility-level tasks • NO review of QI/QM reports
TASK 2: ON-SITE ENTRANCE CONFERENCE • Team Coordinator announces survey and introduces team • Immediatelyobtains an alphabetical resident census with room number, unit, date of birth, and list of residents admitted within last 30 days that reside in the facility
TASK 2 ON-SITE ENTRANCE CONFERENCE - continued • Provide signs announcing the survey; to be posted by facility • Obtain a copy of the facility plan • Explain private interviews will be conducted with residents/families • Team will communicate throughout survey and request assistance as needed - NO DAILY MEETINGS • Conduct complaint investigation during the survey, if applicable • List of residents who receive dialysis, on ventilator, on hospice services
TASK 2 – Concurrent Activities • Tour • Begin process of finalizing Stage I sample • INITIAL KITCHEN/FOOD SERVICE OBSERVATION WHILE OTHER MEMBERS ARE GATHERING INFORMATION • Schedule time to meet and interview Resident Council President and review meeting minutes
TASK 2 – Concurrent Activities • DINING OBSERVATION (starts with first meal that can be observed in full) • MUST IDENTIFY EMERGENCY WATER SOURCE/SUPPLY • MUST PROVIDE SCHEDULE OF MEAL TIMES AND LOCATION OF ALL DINING ROOMS
TASK 3: INITIAL TOUR • Obtain BRIEF overall impression of the facility and the resident population • Meet as many staff/residents/families as possible • NOT a method of sample selection • Record egregious resident care situations to be investigated further in Stage II • Document concerns with environment (dining room, cleanliness, smells, etc.) • Ask staff to identify family members that visit regularly
TASK 3: INITIAL TOUR - continued • Observe staff/resident interactions (privacy and dignity) • Observe staff availability • Observe activities in progress • Observe characteristics of resident populations, i.e. residents with dementia, rehabilitation, and sub-acute clinically complex residents, residents with special care needs (feeding tubes, ventilators, intravenous fluids/medications, tracheostomy tubes, oxygen therapy)
TASK 4: SAMPLE SELECTION • Quality Indicator Survey Data Collection Tool (QIS DCT) provides a systematic automated resident sampling process. • QIS DCT generates 3 Stage I samples from the resident pool • 1) MDS sample • 2)Admission sample • 3)Census sample (subset of resident pool) • Surveyors may generate a non-random, surveyor-initiated sample (subset of resident pool).
TASK 4: MDS SAMPLE REVIEW • Residents whose data trigger the MDS-based Quality Care Indicators (QCIs) will be reviewed in Stage II.
TASK 4: ADMISSION SAMPLE REVIEW • Focus is on quality of care within first six months for short stays • Focal points: Nutrition, Rehab, Skin Care • Record review only • Mostly closed records reviews
TASK 4: ADMISSION SAMPLE REVIEW - continued • WEIGHT LOSS ANALYSES • SURVEYORS ARE INSTRUCTED TO USE SAME CHARTING DOCUMENTATION SOURCE FOR ALL WEIGHTS, IF POSSIBLE. • FOR EXAMPLE, MARS, TARS, DIETARY, NURSING NOTES, WEIGHT/HEIGHT RECORDS. MDS IS LAST RESORT. • SAMPLE SIZE UP TO 30
TASK 4: CENSUS SAMPLE REVIEW • Focus on care of residents currently residing in the facility and encompasses activities of daily living, NUTRITION, medications, ELIMINATION/incontinence, resident room, oral health, quality of life, SKIN CARE • Data collection through observations, interviews, record reviews • Sample size - 40 residents currently residing in the facility
TASK 4: CENSUS SAMPLE REVIEW - continued • Collect and record resident specific information which takes into account situation, time, and multiple observations • Set of prescribed questions to review the initial quality assessment of sample residents and facility (see CMS forms on website) • Includes gathering of sample residents’ specific information by observations, interviews and record reviews
TASK 4: CENSUS SAMPLE REVIEW - continued • This information will be comprehensively analyzed in Stage II. • Observations concerning compromised quality of care of sampled and non-sampled residents are recorded on surveyor worksheets for further survey or review in Stage II.
TASK 4: CENSUS SAMPLE REVIEW - continued • Expect first several days to include a lot of surveyor observations • Surveys are lasting 5 days in Florida • Florida trend - More cites, less severity, more collateral tags
TASK 4: CENSUS SAMPLE REVIEW - continued • Surveyors ask questions as written • Select families from various units • Conducted with family or representative that knows the resident and facility’s care well (3 different families/representatives) • Concerns identified need to be investigated immediately, with the family present (see Attachment A).
TASK 4: CENSUS SAMPLE REVIEW - continued Family and Resident Interviews • Surveyor questions to Family/Representatives: • Does the facility honor the resident’s desires and preferences? • Does the resident get assistance with meals? • What is the food like here? • Are you able to participation in making decisions regarding food choices/preferences?
TASK 4: CENSUS SAMPLE REVIEW - continued Family and Resident Interviews • Surveyor questions to Residents • Is the food appetizing and does it taste good? • Is food served at the proper temperature? • Are you offered fluids between meals? (See Attachments A & B)
Resident Food Choices: Facilitates Cultural Dining, Customer Satisfaction, and Successful QIS Results • Resident Choice Menu Development • Dessert Cart • Soup Cart • Salad Choice • Bread Basket at Table • Beverage Cart • “Room Service” via carts on floor for Room Trays
TASK 4: CENSUS SAMPLE REVIEW - continued Staff Interviews • Conducted with licensed staff (RN/LPN) • Nurse must have frequent and direct contact with the resident • Convenient for the staff • Document what is stated, even if information contradicts information gathered from another source (observation or record review)
TASK 4: CENSUS SAMPLE REVIEW - continued Staff Interviews • Question B1: Nutritional supplement, requires facility documentation of a recording and monitoring system (check or %) • Must show surveyors this documentation. (See Attachment C)
TASK 4: CENSUS SAMPLE REVIEW - continued Clinical Record Review • Encompasses pressure ulcers, psychotropic medications, and weight loss • Conduct record reviews on the unit to continue observations of activities and staff-resident interactions.
TASK 4: SURVEYOR-INITIATED SAMPLE • Chosen by a surveyor at his/her discretion, to be further evaluated during Stage II • Based on resident-specific information obtained from complaints, observations, interviews • Example: dependent diner with a Stage I pressure ulcer who is not being fed and family has verbalized complaints
TASK 4: NUTRITION/HYDRATION/ TUBE FEEDING QUALITY OF CARE INDICATORS USING SAMPLED RESIDENTS • Hydration • Sources - Resident and staff interviews and observations, MDS • Do you have access to fluids? • Do you receive fluids between meals? • Does the resident show signs of dehydration, such as cracked lips, etc.? • Prevalence of dehydration - output exceeds input (from MDS)
TASK 4: NUTRITION/HYDRATION/ TUBE FEEDING QUALITY OF CARE INDICATORS USING SAMPLED RESIDENTS - continued • Nutrition – • Sources – MDS, medical records, staff interviews, observations, chart • Prevalence of weight loss (MDS) • Prevalence of significant weight loss that exceeds the interpretive guidelines (MDS/Medical records) • Excludes residents with terminal illness and on planned weight loss program • Weight loss since admission: 5% unplanned weight loss of 5% or more within 60 days of admit (MDS/Chart) • No supplements and resident underweight (Observation/chart) • Staff interview: Is the resident receiving a nutritional supplement defined as a high calorie/high protein product with or between meals?
TASK 4: NUTRITION/HYDRATION/ TUBE FEEDING QUALITY OF CARE INDICATORS USING SAMPLED RESIDENTS - continued • Tube Feeding • Sources – MDS/Chart • Prevalence of tube feeding (MDS) • Significant weight loss on tube feeding (MDS/Chart)
TASK 4 : RELEVENT FINDINGS • Document observed problems • Document areas of concern • Document date, time, and source • Document person interviewed and title • IDRs will be difficult
TASK 5: FACILITY-LEVEL SURVEY AREAS Survey tasks to be completed: • Demand billing • Dining observation (see attachment D) • Infection control • Kitchen/Food Service Observation (see attachment E) • Med Pass
TASK 5: FACILITY-LEVEL SURVEY AREAS - continued • Nursing services, sufficient staffing* • Personal funds* • QAA Review • Resident Council president interview • Abuse prohibition review* • Admission, transfer, discharge review* • Environmental Observations *completed only if triggered by complaints or Stage I interviews, observations or record reviews.
TASK 5: DINING OBSERVATION • Focuses: enough staff, positive dining experience, residents’ choice • Begins with the first full meal that occurs after the team enters the facility (see handout) • If concerns identified, watch a different meal to see if problem exists during that meal
TASK 5: DINING OBSERVATION - continued • If more than one dining room, observe all dining rooms plus residents dining in-room • If there are problems identified, the surveyor can initiate the full dining observation at any point • Focus on residents who require the most assistance. (See Attachment D)
TASK 5: DINING OBSERVATION - continued • Dining observations will also occur during Stage II for sampled residents with nutrition-related concerns, such as weight loss, decline in eating ability, or dehydration, using the nutrition critical pathway • Names of residents observed not receiving needed services, positioning, or adequate assistance will be recorded on the dining room worksheet to further investigate in Stage II.
TASK 5: DINING OBSERVATION - continued • Family and residents with dining concerns should be documented for private follow-up. Interviews will be conducted. • If surveyor identifies concerns (e.g. resident complaints or high prevalence of unintended weight loss), surveyor may request sample tray (same process as current procedure)
TASK 5: DINING OBSERVATION - continued • Test tray will be sent to unit the furthest distance away • Test tray is to be done when the last resident is served. If concerns are identified, such as F371 or F364 - unpalatable food or at improper temperatures or unsanitary conditions, the surveyor is to initiate the appropriate tag and document concerns in the computer to address further in Stage II
TASK 5: DINING OBSERVATION - continued • Multiple meal observations through survey • Work sheet entered in computer during Stage II
TASK 5: DINING OBSERVATION - continued Examples of Questions on Dining Observation Tool: • Are staff members assisting with dining at scheduled times, providing timely and appropriate assistance? • Are staff members talking with residents? • Are staff members allowing residents adequate time to eat? • Are meal substitutes offered when meals are refused?
TASK 5: DINING OBSERVATION - continued • Are residents positioned to maximize eating abilities? • Are dining rooms free of offensive odors? • Does staff utilize hygienic practice? • Does the facility offer sufficient liquids with meals? • Does the facility serve meals in an attractive manner? • Are residents’ desires taken into account when using clothing protectors? • Are adaptive devices utilized to promote independence? (See Attachment D)