Download
1 / 49
720 likes | 2.13k Views
ASTIGMATISM. ASTIGMATISM: PROGRAM. Astigmatism: program. Definition Epidemiology Classification Symptoms and signs Methods of measurement Prescription criteria Resolution of clinical cases. ASTIGMATISM: DEFINITION. Astigmatism: definition .

E N D
Astigmatism: program • Definition • Epidemiology • Classification • Symptoms and signs • Methods of measurement • Prescription criteria • Resolution of clinical cases
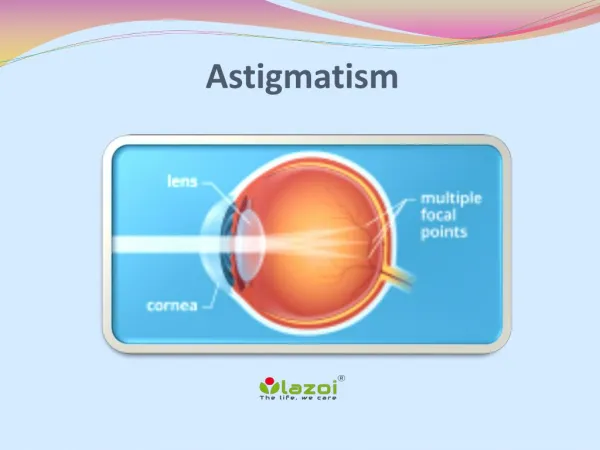
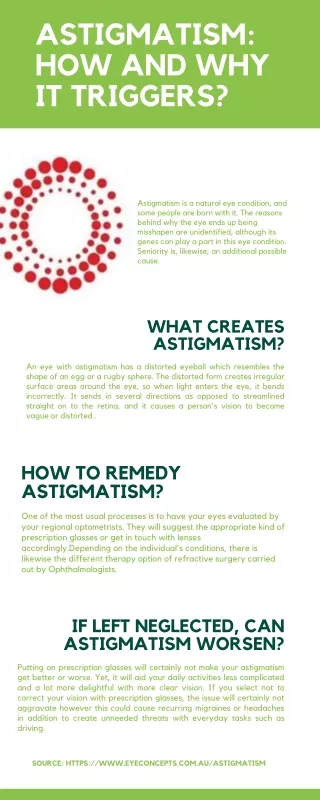
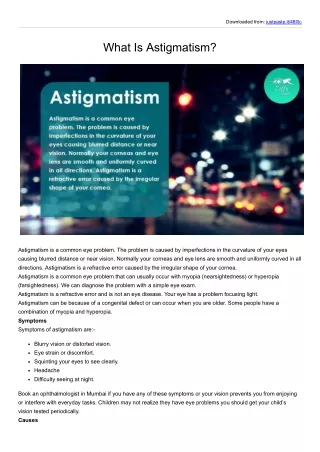
Astigmatism: definition • Refractive condition in which the image of an object is not formed on a solo plane, since the different ocular meridians are of distinct potency (distinct focal distances). • Habitually, there are 2 main meridians, of maximum and minimum potency, and perpindicular to one another.
Astigmatism: epidemiology I • The majority of eyes show weak astigmatism. • Astigmatism can present itself in an isolated form or, with greater frequency, associated with myopia or hypermetropia. • Between 2-6% of the population has an astigmatism > 2,00 dioptre
Astigmatism: epidemiology II • Changes with age • An significant percentage of newborns show inverse astigmatism. • During the first few months of life the astigmatism dimishishes gradually. • At school age, direct astigmatism of low magnitude tends to exist. • Throughout youth and adulthood, astigmatisms do not tend to pass through any important changes. • From the 50-60 and on, increases in inverse astigmatism or decreases in direct astigmatism exist.
Astigmatism: epidemiology III • Genetics • In corneal astigmatisms >1,50/2,00D there is a strong genetic component • Environmental factores • The use of rigid contact lenses can induce variations in the corneal astigmatism of 2 or more dioptres. • Various authors suggest that astigmatism and its variations are the consequence of the relationship between the palpebral tarsus and the cornea.
Astigmatism: classification I • According to the regularity of the corneal surface • According to the direction of the main meridians • According to the refraction of the eye
Astigmatism: classification II • According to regularity of the corneal surface • Regular (habitual): • Main meridians are perpindicular to one another • Irregular (infrequent): • Main meridians are not perpindicular • Curvature of one of the meridians is not constant Irregular corneal astigmatism Regular corneal astigmatism Spherical cornea
90° 70° 110° 135° 45° 160° 20° 0° 180° Astigmatism: classification III • According to the direction of the main medians of the astigmatism of the eye • Direct astigmastism or “in favor of the rule” • The horizontal meridian is the flattest • The horizontal meridian is less powerful • The axis of the refractive astigmatism, expressed in negative potency, is around 0º-180º (±20º) • It is the most frequent
90° 70° 110° 135° 45° 160° 20° 0° 180° Astigmatism: classification IV • According to the direction of the main meridians of the astigmatism of the eye • Inverse astigmatism or “against the rule” • The vertical meridian is the flattest • The vertical meridian is less powerful • The axis of the refractive astigmatism, expresed in negative potency, is around 90º (±20º)
90° 70° 110° 135° 45° 160° 20° 0° 180° Astigmatism: classification V • According to the direction of the main meridians of the astigmatism of the eye • Oblique astigmatism • The main meridians are between 20° and 70° and between 110° and 160°
Astigmatism: classification VI • According to the refraction of the eye: • Simple: only one meridian is ametrope (only astigmatism exists). • Example 1: -0,50x90º (simple myopic astigmatism) • Example 2: +1,25x5º (simple hypermetropic astigmatism) • Compound: the two meridians show the same type of ametropia. • Example 1: +2,50+1,75x15º (Compound hypermetropic astigmatism) • Example 2: -1,00-0,75x30º (Compound myopic astigmatism) • Mixed: the two meridians are ametropic and of a different type. • Example 1: +0,50-1,50x10º (the potency of one meridian is +0,50 and the other -1,00)
Simple H. Astig. Compound H. Astig. Simple M. Astig. Compund M. Astig. Mixed Isodioptric Astig. Mixed Isodioptric Astig. Astigmatism: classificaction VII • In the following schemes the formation of images in the retina according to the eye’s refraction are shown:
Optical cross: The weaker meridian (flattest) is the one at 180º Transposition formula: +1,50+2,00x90º Classification according to main meridians: Direct astigmatism Classification according to refraction: Compound hypermetropic astigmatism +3,50-2,00=+1,50 +3,50 Astigmatism: classification VIII Example 1: +3,50-2,00x180º
Astigmatisms: symptoms and signs I • The symptoms tend to depend on the magnitude of the astigmatism. • Moderate and evelated astigmatism • Blury vision in DV and NV • Symptoms of visual fatigue, headache, ocular irritation, etc. • Symptoms of image distortion and absence of comfort upon initial use of lenses that compensate for astigmatism
Astigmatisms: symptoms and signs • Low astigmatism (<1,50D) • The VA does not tend to be very affected, but it is difficult to determine it precisely • Visual fatigue associated with prolonged use of vision • Inverse astigmatisms tend to produce greater symptomology than direct ones • Significant difficulties to adapt to the new prescription do not tend to appear
Astigmatisms: symptoms and signs III • Imprecision in the determination of VA • Low astigmatisms < 1.50 D • If it is hypermetropic the VA can easily reach 20/25 or even 20/20 • If it is myopic the VA is affected more and is near 20/30 • Moderate to high astigmatisms (≥1,50-2,00 D) • If it is hypermetropic the VA is diminished, but not as much as it would be if it were myopic • If it is hypermetropic the diminishment of the VA will be ≈ in DV and in NV • If it is myopic the diminishment of the VA will be greater in DV than in NV • Oblique astigmatisms demonstrate the worst VA • Comparing the same level, the VA in the oblique astigmatism < VA in inverse astigmatism < VA in direct astigmatism
Astigmatism: methods of measurement I • Keratometry: determination of the power of the main meridians of the cornea • Hemholtz • Javal • Automatics • Corneal topography: determination of the morphology of the anterior corneal surface
Astigmatism: methods of measurement II • Keratometry: • Clinical technique to measure the radius of the curvature of the anterior face of the cornea. • Based on the reflection of light in the cornea (convex mirror). It gives a small image, straight and virtual, of the object (“look”) which is of a known size • The measurement is done in a diameter of 3 mm around the visual axis
Astigmatism:methods of measurement III • Hemholtz’s keratometer • Javal’s keratometer • Automatic keratometers
Astigmatism: methods of measurement IV • Corneal topography: • Can measure large areas • Is a quantitative evaluation • High resolution (approx. 5000 puntos) • Lots of presentation options
Astigmatism: methods of measurement V • Clinical use • Informs on the quality/integrity of the corneal surface • regular : clear and regular vision and the main meridians are perpindicular • Irregular: irregular or distorted vision. The precise determination of the main meridians is difficult • Help in the determination of approximante astigmatic refraction • In cases of minimal collaboration • When ocular means are unclear • Essential help in the selection of parameters for contact lenses
Astigmatism: methods of measurement VI • Limitations of keratometry: • An astigmatism determined through keratometry corresponds to the anterior face of the cornea. • Astigmatism also exists in the posterior face of the cornea, being crystalline and even retinal. • The design of the keratometer is based on spherical surfaces and this leads to errors in the measurement • The visual axis frequently remains displaced from the geometric center of the cornea • The measurement is done is a 3 mm diameter around the visual axis
Astigmatism: methods of measurement VII • The total astigmatism (TA) is the sum of: • Astigmatism of the anterior face of the cornea (FHC) • Internal physiological astigmatism (IPA) • Javal’s rule: • In general, the IPA has an approximate value of -0,50x90º • Example 1: • FHC = -1,75x180º • Which TA is expected, if we follow Javal’s rule?
Astigmatism: prescription criteria I • Age of the patient: • Small children (from 2 to 6): total compensation if the VA is believed to be compromised. There tends to be good tolerance. • Children (from 6 to 12): total compensation continues being recommended, but the tolerance tends to lessen. • Adults: Variable tolerance to the changes: • If there are great improvements of the VA: prescribe for the astigmatism • Oblique axes: partial compensation of the astigmatism
Astigmatism: prescription criteria II • Magnitude of the astigmatism: • The greater the astigmatism, the lesser the tolerance to the total prescription • Elevated astigmatisms tend to be congenital or of early appearance. If no prescription is made, they can provoke ambyopia. • In cases of irregular elevated astigmatisms the best VA is obtained through the use of rigid contact lenses. • Small astigmatisms (<1,00D) do not tend to require serious consideration.
Astigmatism: prescription criteria III • Habitual astigmatic prescription: • When an adult patient does not show symptoms with his/her habitual compensation, it seems wise not to realize important changes. • Consider changes when symptoms, marked reduction of the VA or reduction of stereopsis exists. • For adults that have never had astigmatism: • Reduce the cylindrical power, maintaining the spherical equivalent. • With the passage of time try to align the level of prescription to the refraction of the person.
Astigmatism: prescription criteria IV • Method of the spherical equivalent (SE) • Method to reduce the power of the cylinder but allowing that, without additional accomadative force, the circle of least confusion is situated over the retina. • Half of the magnitude of the unprescribed cylinder (SE) sums up algebraically to the value of the sphere • Example 1: +2,50-3,50x85º • 2,00 dioptres are prescribed • SE of the unprescribed astigmatism = -1,50/2 = -0,75 • The SE adds up to the value of the sphere: +2,50 +(-0,75) = +1,75 • Final prescription: +1,75-2,00x85º
Astigmatism: case 1-I • MJH, 12-year-old child. Student. • MC: Occasionally shows that he does not see well in NV. Visual tiredness when studying. Occasional ocular hyperaemia. • PH: Has never worn glasses. Previous pediatric check-ups. No illnesses or ingestion of medication. • FH: Unimportant.
Astigmatism: case 1-II • Habitual VA in DV and NV: • RE: 20/20-2; NV: 20/25 • LE: 20/25; NV: 20/25 • Binocularity in habitual conditions: • Cover test: • DV: ortho • NV: ortho • Proximal convergence: 5/8cm
Astigmatism: case 1-III • Retinoscopy: • RE: +1,00-1,50x180º • LE: +0,50-1,50x5º • Subjective DV and VA: • RE: +0,50-1,25x175º; VA: 20/20 • LE: +0,25-1,25x5º; VA: 20/20 • NV with the subjective: VA 20/20 in both eyes. Good comfort • Amplitude of accomodation with the subjective: • RE: 8cm≈12,5D • LE: 8cm≈12,5D • Ocular health exams: within normal limits • Color vision: normal
Astigmatism: case 1-IV • Complete diagnostic of the case • Proposed treatment and plan of check-ups • Possible evolution of the condition
Astigmatism: case 1-V • Complete diagnostic of the case • Low hypermetropia present in both eyes • Direct astigmatism in both eyes: • According to the conoid: mixed in both eyes • Binocularity and accomodation: within the normal limits • Other tests within normal limits
Astigmatism: case 1-VI • Proposed treatment: • Glasses with the value of the subjective: • RE: +0,50-1,25x175º • LE: +0,25-1,25x5º • Use mainly for school and work in NV. • They can be worn for all uses. • Revision in one year or before if new symptomology appears. • Explain the condition to the patient and his/her parents.
Astigmatism: case 1-VIII • Possible evolution of the condition: • Stability of the stigmatism • Slight diminishment (or stability) of the hypermetropia
Astigmatism: case 2-I • JJB, 25-years-old. Waiter. • MC: Notices sporadic diminishment of vision, as much in DV as in NV. Greater difficulty at the end of the day. • PH: 15 years ago he was prescribed glasses but they were very uncomfortable and he never wore them. No illnesses or ingestion of medication. • FH: Irrelevant.
Astigmatism: case 2-II • Habitual VA in DV y NV: • RE: 20/40; NV: 20/40 • LE: 20/30; NV: 20/25 • Binocularity in habitual conditions: • Cover test: • DV: ortho • NV: ortho • Proximal convergence: as far as the nose
Astigmatism: case 2-III • Retinoscopy: • RE: +3,00-4,00x5º • LE: +1,50-2,50x20º • Subjective DV and VA: • RE: +2,75-3,50x5º; VA: 20/25 • LE: +1,00-2,00x15º; VA: 20/20+ • DV and NV with the subjective: notices better vision but is not comfortable. A reduction of the graduation is tried and tolerance is greater: • RE:+2,00-2,00x5º; VA: 20/25-2 • LE: +0,75-1,50x15º; VA: 20/20 • Amplitude of accomodation with the second refraction: • RE: 14cm≈7D • LE: 11cm≈9D • Exams of ocular health: within normal limits • Central fixation in both eyes
Astigmatism: case 2-IV • Are other tests necessary for a correct diagnosis and treatment? • Complete diagnosis of the case • Proposed treatment and plan of check-ups • Possible evolution of the condition
Astigmatism: case 2-V • Are other tests necessary for a correct diagnosis and treatment? • VA with a stenopaic disc? • Keratometry?
Astigmatism: case 2-VI • Complete diagnosis of the case • Hypermetropic and astigmatic anisometropia • Hypermetropia becomes apparent in both eyes (RE>LE) • Direct astigmatism in both eyes (RE>LE) • According to the conoid: mixed astigmatism in both eyes • Slight amblyopia in the RE • The rest of the tests within normal limits
Astigmatism: case 2-VII • Proposed treatment: • Prescribe glasses with the determined equivalent: • RE:+2,00-2,00x5º • LE: +0,75-1,50x15º • Use as much in DV as in NV. • Explain the condition to the patient • New revision in 3-4 months
Astigmatism: case 2-VIII • Possible evolution of the condition: • Significant changes to the value of the refractive defect are not expected in the first few years • Periodical check-ups are necessary since we want to get the prescription as near as possible to the value of the refractive defect • Greater dependence on glasses with the passage of time
Astigmatism: bibliography • Amos JF. Diagnosis and management in vision care. Butterworth-Heinemann, 1987 • Grosvenor T, Flom MC. Refractive anomalies. Research and clinical applications. Butterworth-Heinemann, 1991 • Brookman KE. Refractive management of ametropia. Butterworth-Heinemann, 1996 • Werner DL, Press LJ. Clinical pearls in refractive care. Butterworth-Heinemann, 2002
Astigmatism: Bibliography • http://en.wikipedia.org/wiki/Astigmatism • http://www.healthatoz.com/healthatoz/Atoz/ency/astigmatism.jsp • http://www.eyemdlink.com/Condition.asp?ConditionID=250