Download
1 / 61
620 likes | 683 Views
Functional disorders. Updated July 2016. Goals. I. Define functional disorder in adolescents and the impact on adolescent biopsychosocial development II. Demonstrate knowledge of epidemiology, aetiology and pathogenesis of functional disorder in adolescence

E N D
Functional disorders Updated July 2016
Goals I. Define functional disorder in adolescents and the impact on adolescent biopsychosocial development II. Demonstrate knowledge of epidemiology, aetiology and pathogenesis of functional disorder in adolescence III. Demonstrate skills in assessment and diagnosis of functional disorder during adolescence IV. Demonstrate proficiency in developing and implementing a management plan for an adolescent with a functional disorder, involving them, their parents and the wider network
I. Define functional disorder in adolescents and the impact on adolescent biopsychosocial development
Definitions DSM-V somatic symptom disorder • Experiencing exaggerated and disrupted physical symptoms • Exaggerated thoughts impairing activities of daily living • Last > 6 months • Includes adolescents with chronic conditions
Definition: pain Pain: noxious sensation in the body suggesting tissue damage (bio-medical) Suffering: experienced by a person (not body); arises from threats to the intactness of the person as a complex social and psychological entity Suffering= Pain X Resistance
Definition: chronic pain • >3 months • Impact on adolescent daily life and functioning • Can be related to underlying chronic condition or idiopathic/functional
Localised Complex Regional Pain Syndrome 1 Complex Regional Pain Syndrome 2 Reflex Sympathetic Dystrophy Sudek’s Atrophy Shoulder-hand Syndrome Post-traumatic pain syndrome Algodystrophy Causalgia Phantom pain Recurrent headaches/abdominal pain/chest/pelvic pain Diffuse Juvenile Fibromyalgia Pain Amplification syndromes Post Viral Syndrome M.E Chronic fatigue/pain Idiopathic Pain Syndromesduring Adolescence Pain Associated Disability Syndromes
The Purpose of Pain • The purpose of pain is not to act as a damage meter but as a motivational driver for protection (Moseley 2007, Williams 2011) • Pain closely associated with fear and stress responses as part of a protective mechanism • Threat is not necessarily real, the brain may be mis-interpreting signals (? stress) as ‘a threat’ leading to a pain response.
Social Within the family Within the peer/friendship group Exploratory behaviours Vocational development • Biological • Secondary sexual characteristics • Reproductive capacity • Growth spurt • Bone density • Brain development Psychological Self concept Concrete/Abstract Thinking Body Image Chronic Pain
Using the grid for support, consider the impact of a functional disorder on adolescent developmental goals Adapted from WHO publications
Define main developmental goals of early, mid and late adolescence using the grid as support
Reported Sequelae of Pain • (H) • E – Education 48.8% school absence • A – Activities 53.3% inability to pursue hobbies; 46.7% inability to meet friends • D – Diet 51.1% eating problems • S – Sleep problems 53.6% Roth-Isigkeit A et al, 2005
II. Demonstrate knowledge of epidemiology, aetiology and pathogenesis of functional disorder in adolescence
Multiple health complaints@ 15 years www.hbsc.org (2013/2014 survey)
Multiple Health Complaints www.hbsc.org.uk, England 2014 survey
Epidemiology of Chronic Idiopathic Pain • 15% paediatric population • Mean age at onset 12-13 years • 4F:1M • Most have constant pain • Most have multiple pain • LL > UL • Common cause of school non-attendance • Can complicate other illnesses eg Juvenile Idiopathic Arthritis, inflammatory bowel disease, cerebral palsy, sickle cell, cancer
Epidemiology of Pain N=749 school children (83% 10+ yrs) • 83% pain in last 3months • 30.8% pain present > 6months • Headache 60.5% • Abdominal pain 43.3% • Limb pain 33.6% • Back pain 30.2% • 50.9% sought professional help • Two thirds reported restriction in ADLs Roth-Isigkeit A et al, 2005
Somatoform paradigms Conditioned responses … cause symptoms to be perpetuated in the absence of stimuli Triggers Multiple precipitants of symptoms Reflexes Autonomic, involuntary, subcortical Autonomic Nervous Systems Balance of sympathetic vs parasympathetic
Neuroscience Advances • Rapidly changing field! • Growing evidence that the brains of people with chronic pain are different at a functional, structural and molecular level Eg Woolf 2010; Apkarian 2010 • Reversible • ? Consistent across life course • ? cause or effect
The Pain Neuromatrix The combination of cortical mechanisms that when activated, produce pain Moseley 2003 Activated by both nociceptive and non-nociceptive (cognitive, beliefs and attitudes) mechanisms conviction of the CNS that body tissue is in danger and under threat. Whilst threat remains, so will the pain. Therefore we need to help the patient reduce the threat
Country lanes and Motorways! Pain pathways when used repeatedly become more ‘slick’. Increased pain traffic can turn a country lane into a motorway Results in signals from the painful area being carried much more efficiently
Central sensitisationExplanations Car alarm – Gust of wind sets it off Body Thermostat – is set lower, therefore pain comes on at a lower level of stimulation Burglary – Burglar breaks in damaging the window (tissue damage) and sets off alarm. Police come and arrest the burglar. Owner can’t find a way to turn off the alarm (pain persists). People respond to a burglary in different ways – some not bothered, some never want to go into the house again.
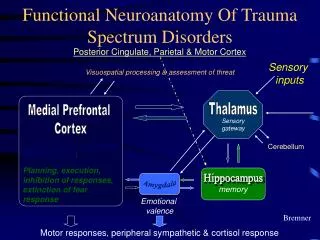
Effect of stress on the body • Prolonged stress leads to wear-and-tear on the body (Allostatic load) • Mediated through the sympathetic system • Allostatic load leads to: • Impaired immunity, atherosclerosis, metabolic syndrome, bone demineralisation • Atrophy of nerve cells in the brain (hippocampal formation (learning/memory) and prefrontal cortex (working memory/executive function) • Growth of amygdalia mediates fear response • McEwen BS, Ann N.Y Acad Aci 2004
Relationship between stress and performance The Yerkes-Dodson Law, 1908
Why the high prevalence of functional disorder during adolescence? Ability to express emotions is evolving with the maturation of the brain Body changes are a main concern Autonomy is a central task and can be threatening for adolescent/parents
III. Demonstrate skills in assessment and diagnosis of functional disorder during adolescence
Making the Diagnosis • History • Examination
History-taking NB A thorough assessment can be a good intervention From the outset, start linking the functional symptom eg pain to psychological symptoms ‘When you get the pain, what emotions come with it?’
Assessment • Symptom itself eg Pain • Activities of Daily Living ADL (Typical day- week vs weekend) • HEADSSSS • Stressors & personal barriers • Risk and resilience • Coping strategies • Beliefs • Understanding and acceptance of diagnosis • Motivation • Symptom spider…
Think of a young person with a functional disorder and imagine what aspects of their lives they would use to create their symptom spider… Symptom eg pain
Example of a Symptom Spider social life sleep family Symptom appetite /eating school independence fitness mood
Consultation Strategies • Agenda setting • Acknowledge mismatching agenda • Turn taking • Involve each member in turn • Open > closed questions • Check understanding “Did you say…” “As far as I heard….” • Miracle Question • If you each could change one thing, what would it be…..? • What do you think is wrong? Are you worried it might be something in particular? • Ask about variability. What makes for a better day?
When to Worry • Co-occurrence of multiple symptoms • Chronicity > 3 months • School attendance • Isolation • Recent family, school, psychological problems
Sleep disturbance in Chronic Pain Syndromes • go to bed late • unable to get to sleep • wake through night due to discomfort • increased motor agitation during sleep • fatigue on waking • “Sleep clock” abnormalities • nocturnal eating • interferes with life
Clues from History • Increasing pain after minor trauma • Marked disability • Worse with rest • Failed prior therapy • Autonomic symptoms (temperature/colour changes, perspiration) • Prior episode of pain • “Slow healer” • Hypervigilance (and protracted system review!) • Other pains eg headache, abdominal pain
General Enmeshment with parent Spokes-parent Pseudo-mature Incongruent affect La belle indifference Compliant Specific Hypermobility Allodynia Anticipatory pain Wince and withdrawal Soft tissue swelling Autonomic signs – colour/temp change, sweating, hair growth *Check after exercise, when dependent as may be more obvious Bizarre posture Bizarre/energy rich gait Clues from examination
The Diagnosis This should be a positive event! Invest time Legitimise condition Tell them how common it is. Explain the vicious spiral……… Dismiss the trigger. Explain pain pathway.
Useful Statements The pain is real. I believe you. You are not faking it, putting it on etc. You are not mad. You have a genuine condition. This is entirely treatable Consider if you bang your thumb with a hammer…Bang thumb – physical…How do you feel? Angry – psychological
‘Pain does NOT always = damage’ Consider a paper cut …Extremely painful but very little tissue damage Consider stubbing your toe… Even more painful, but very little damage Grip your hand very tight - hold it for a few minutes - then relax. Do you feel the ache....
Giving the DiagnosisHelpful hints • Useful vs not useful pain • Subjective swelling - thick lip at the dentist • Phantom Pain (pain memory) • Battlefield injuries • Vicious spiral
IV. Demonstrate proficiency in developing and implementing a management plan for an adolescent with functional disorder involving them, their parents and the wider network
Management: General Principles • Time++++ • Exclude other diagnosis but know when to STOP investigating/referring • Avoid manipulation • Multidisciplinary • Consistency of approach within team and caregivers • Documentation
Management • Multidisciplinary • Education/reassurance/confidence • Goal setting • Graded activity programme • Pacing • Anxiety management/Relaxation. • Sleep hygiene • Coping strategies. • Desensitisation • Relapse prevention • Time table of daily routine • Written contracts • Homework • Psychology referral • School reintegration
Pain Spirals From www.paintoolkit.org
Can I have another scan? If I were to scan your head when you had a headache - it would be normal BUT the pain would still be there School with damaged roof. Taking a photo will show damage BUT could you tell if it was a good school, what the students are like? Scans do not necessarily give you the information you actually want to know
The Diagnostic VacuumRisks of Over-investigation and Poly-doctoring! • anxiety • uncertainty • confidence
Management of functional disordersFrom vicious circle to virtuous circle
Symptom Spiders • Non-standardised assessment and goal setting strategy • Multidisciplinary team focus • Holistic strategy to suit a broad client group • Symptom spiders helps to prioritise short term goals and long term goals. • Visual concrete item to help individuals focus • Builds rapport and opens up communication.