Download
1 / 67
670 likes | 764 Views
Minnesota e-Health Summit, June 16, 2011 Beacon Overview - Lacey Hart, MBA, PMP®. Demonstrate a vision of the future where: Hospitals, clinicians, & patients are meaningful users of health IT

E N D
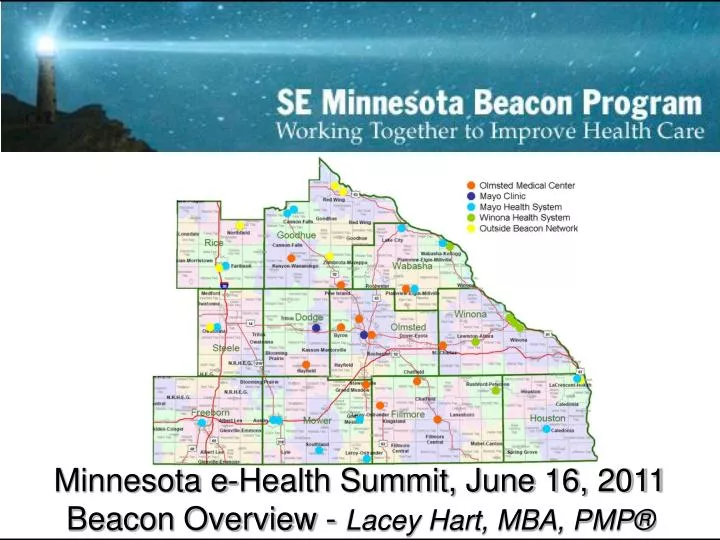
Minnesota e-Health Summit, June 16, 2011 Beacon Overview - Lacey Hart, MBA, PMP®
Demonstrate a vision of the future where: • Hospitals, clinicians, & patients are meaningful users of health IT • Communities achieve measurable & sustainable improvements in health care quality, safety, efficiency, and population health Extend advanced health IT & exchange infrastructure Leverage data to inform specific delivery system & payment strategies 2
17 Beacon Communities • Louisiana Public Health Institute, New Orleans, LA • Southeast Minnesota, MN • Rhode Island Quality Institute, Providence, RI • Rocky Mountain Health Maintenance Organization, Grand Junction, CO • Southern Piedmont Community Care Plan, Inc., Concord, NC • The Regents of the University of California at San Diego, San Diego, CA • University of Hawaii at Hilo, Hilo, HI • Western New York Clinical Information Exchange, Inc., Buffalo, NY • Community Services Council of Tulsa, Tulsa, OK • Delta Health Alliance, Inc., Stoneville, MS • Eastern Maine Healthcare Systems, Brewer, ME • Geisinger Clinic, Danville, PA • HealthInsight, Salt Lake City, UT • Indiana Health Information Exchange, INC., Indianapolis, IN • Inland Northwest Health Services, Spokane, WA 3
SOUTHEAST MINNESOTA BEACON • KEY PARTNERS: • County Public Health • Mayo Clinic Rochester • Mayo Health System • Olmsted Medical Center • Public School Systems • Winona Health System “New Model of Care” Improved Patient Care Quality Improved Care Efficiency Population Health Management Effective Payment Delivery Sustainable Regional ‘Practice’ ROADMAP • Population Health Data • Best-Practices Discovery • Improve Clinical Quality • Asthma Management • Diabetes Management • Reimbursement Modeling Mobilize & Align Region Community Engagement Technology Infrastructure Data Exchange Adopt National Standards 4/2010-3/2011 4/2011-3/2012 4/2012-3/2013 4
Southeast MN BEACON GOALS • Laying the groundwork for better use of health information to improve health • Demonstrate secure, confidential health information exchange between parties authorized by the patient • Reduce inappropriate healthcare utilization and cost • Improve the ability of individuals to follow through on disease treatment plans 5
“Ultimate Aim” Establish SE MN as “the premier population-based laboratory for healthcare delivery, best-practices discovery, reimbursement modeling, clinical quality optimization, and translational research in the country.” 6
SE MN Beacon Organization Dept. of Health & Human Services (DHHS) Federal Steering Committee (FSC) - TBN Office of the National Coordinator of Healthcare IT (ONC) Community Interest Groups National Beacon Communities Evaluation MN Congressional Offices SE MN Beacon Governance Approval to Execute SE MN Healthcare REOT Winona Health Leadership Public Health Leadership Olmsted Medical Leadership Mayo & Mayo Health System Leadership CPC CPQOC SE MN Public Health Planning Process Stakeholders Operations Communications Subject Matter Expert WGs Program Management Infrastructure Metrics Comparative Effectiveness SE MN Schools Project Initiation Process Practice Implementation Community & PH Engagement Quality Academy Others Cross Beacon / ONC Projects Project Driven teams Project Execution HIE Connectivity Data Repository Broad- band Mini- deliberative LPH / Schools Asthma Phase 1 Diabetes Phase 1 Immun. Pilot 7
Healthcare Transformation Patient Outcomes IT Enable Knowledge discovery in world of data Satisfy conversations New models 8 8
BEACON HIE Requirements HIE Document Exchange Patient cross-correlations between providers and county healthcare case clients. Pulling CCD, AAP, Care Plan documents to render appropriate patient care. Pulling / Pushing Assessments back to clinicians Establish suite of solutions for various provider capacities (from significant to minimal capacity) 9
Drivers for CDR Driving factors for the repository: Beacon Reporting requirements Population Management Infrastructures/environment & project beyond the grant Provider EMR Systems -> Provider PM Systems Population management in support of meaningful use 10
Healthcare Transformation Patient Outcomes IT Enable Knowledge discovery in world of data Satisfy conversations New models 11
Ensuring the values and preferences of informed patients are brought into our program through meaningful conversation. Guiding Values 12
Creating Conversation to Overcome Lack of Adherence Create a two-way conversation that enables patients to participate in making decisions to the extent they prefer. Medication Choice conversation for a typical patient with Type II Diabetes Courtesy of the Knowledge and Encounter Research Unit at Mayo Clinic in Rochester, Minnesota - Dr. Victor Montori 13
Healthcare Transformation Patient Outcomes IT Enable Knowledge discovery in world of data Satisfy conversations New models 14
Asthma Care Coordination Includes processes of care coordination with providers, public health and schools. 15
Building a Community Dan Jensen, MPH
Community Engagement Vision New Model of Care Accountable Care Organization / High Quality Care Consistent with our efforts for improving care; Beacon facilitate improved clinical work flows Opportunity for Providers to have national visibility as a practice providing “high value” primary care Sustain practice improvements as part of Beacon implementation MN Community Measures / Meaningful Use Resources from REACH and SE MN community support our practice efforts for adoption of technology in a “meaningful manner” Beacon resources for us to advance our cause and undertake clinical research efforts 19
Why is SE MN Beacon important to Public Health? • $ 1.7 million investment in user owned and designed community software operating in all 11 SE MN local public health departments • Lays the groundwork for better data to support local public health community health needs assessment • Increases LPH and practice infrastructure for more effective secure data exchange i.e. communicable diseases • Addresses three local public health responsibilities of Community Health Boards • Assure an adequate local public health infrastructure • Promote Healthy Communities and Healthy Behaviors • Assure the quality and accessibility of health services 20
Why is SE MN Beacon important to Patients (Asthma/Diabetes) • Laying the groundwork for better use of health information to improve health • Demonstrate secure, confidential health information exchange between parties authorized by the patient • Reduce inappropriate healthcare utilization and cost • Improve the ability of individuals to follow through on disease treatment plans
Austin Medical Center Mayo Health System Mayo Clinic Olmsted Medical Center Winona Health Services 22
Community Engagement Challenges in 2011 Positively engaging the community to support record based research and practice improvement Scaling interventions in the region 23
PRO Initiative: Vision, Structure & Progress Dr. Jeff Sloan
The Vision: QOL PROs as an integrated vital sign Patient Clinical profile Patient-reported QOL-related assessment intake Prophylactic interventions for PRO QOL-related domains Treatment Real-time Monitoring of PRO QOL-related domains Triggered supportive care or treatment modification 26 Reduced emergent care Improved survival Improved quality of life
Biomarker Assay (BMA) Positive versus Negative23 trials (3,704 patients) BMA+ BMA- Survival Time (Years) 27
BMA- = a score of 5 or lessin patient-reported QOL on a 0-10 scale This is a reliable and valid measure for cancer patient populations (Sloan, MCP, 2002; Huschka, Cancer, 2005; Locke, JPSM,2007) cut-off validation: Butt, JPSM,2008; Sloan, Value in Health, 2007; Temel, J Thorac Oncol, 2006 28
Clinical Pathway for Overall QOL Deficit Management EVALUATION • Specific QOL domain • deficits 30
PROs in Clinic can be used to: • Find PRO-related problems • Uncover otherwise unknown problems • Modify treatment 31
Case Study #1 • 8 year cancer survivor annual clinic visit • Rated QOL as a 2 out of 10 • Initiated conversation • Insomnia • “stupid thoughts” • Suicidal ideation 32
Case Study #1 • Psych referral • Anti-depressant • 1 month later QOL was 7 33
Beacon PRO Foci • Enhanced monitoring can improve outcomes: • Insulin Control (10%) • Education (50%) • Lifestyle (25%) • Family (35%) • Complications (up to 75%) • Estimates based on DCCT and EDIC trials NEJM, 329,1993 and NEJM 353, 2005 . 34
Asthma Intervention Dr. Erin Knoebel
Asthma Project Team Accurso, Kathy, Rochester Public School Ahern, Lois, Public Health Aleman, Marty, Public Health Baumbach, Shaylene, Public Health Beebe, Calvin E., Mayo Clinic Bock-Goodner, Cynthia, Mayo Clinic Donnal, T. M.D., Winona Health Frazier, Christa, Winona Health Gunderson, Margene, Public Health Hart, Lacey, Mayo Clinic Horton, Ian, Mayo Clinic Jensen, Dan, Public Health • Juhn, Young J., M.D., Mayo Clinic • Knoebel, Erin E., M.D., Mayo Clinic • Lowe, David. M.D.; Olmsted Medical • Martin, Erin L., Mayo Clinic • McWilliams, Deb, M.D., Mayo Clinic • O’Brien, Michael, Mayo Clinic • Naessens, James, Sc.D., Mayo Clinic • Ravikumar, Prajna, Mayo Clinic • Targonski, Paul, M.D., Ph.D., Mayo Clinic • Wellik, Mary, Public Health • Williams, Linda M.D., Olmsted Medical • Yawn, Barbara, M.D., Olmsted Medical 37
School-aged Children: Asthma Prevalence Asthma is estimated - to occur in 7% of school-age children nationally 1 - to occur in 12% of school aged children in Rochester, MN 2 CDC. Surveillance for Asthma --- United States, 1960--1995. MMWR 1998;47[No. SS-1]:1—28 Yawn BP, Wollan P, Kurland MJ, Scanlon P. A longitudinal study of the prevalence of asthma in a community population of school age children. J Pediatrics 2002;140(5):576-581. 38
School-aged Children: Asthma Impact Poorly controlled asthma can affect a child’s ability to exercise, self-esteem, school performance, school attendance. Asthma action plans can decrease preventable illness. National Heart, Lung, and Blood Institute. 2007. National Asthma Education and Prevention Expert Panel report 3: guidelines for the diagnosis and management of asthma. Bethesda (MD): National Institutes of Health. Available from URL: www.nhlbi.nih.gov/guidelines/asthma/epr3/index.htm 39
Collaborative Experience Community Collaborative Asthma Project in Olmsted County (2007 – present) Mayo Clinic Olmsted Medical Center Olmsted County Public Health Rochester Public Schools (ISD#535) Rochester Private Schools 40
Beacon Proposal Extend the asthma action plan model to the 11-county region, augmented with standards-based HIE. Sharing action plans for children with asthma can: Reduce healthcare utilization Improve school attendance Reduce time parent misses work 41
Care Coordination Includes processes of care coordination between health professionals, public health and schools. 42
Asthma Measures Future/Advanced Measures Preventative Care Utilization Appropriate Med Usage Inpatient/ED Utilization Acute attacks in school School Absenteeism Baseline Measures % patients age 5-18 % w/documented Action Plan % w/Influenza Vaccine % w/pneumonia Vaccine % of total ED Visits 43 COST – QUALITY – POPULATION HEALTH
AAP Expansion Project • Leverage lessons learned and tools developed in Olmsted County Asthma Action Plan Task Force providing patient-centered care to ensure anyone who cares for a child with asthma has access to and understands that child’s AAP: • Develop a consent process • Approved by schools and state • Templates are available • Process flow sheets created • SE MN Beacon will expand to ALL school districts: • School System AAP FAQs • Consent Form to Share Asthma Action Plan Template • Consent Form Process Flowsheet Template • School Personnel Education : • Access and understanding of AAPs for ALL personnel • When to Consider communication with the Provider & Parent 44
Technology Pilots • Technology specifications created by the Asthma Action Plan Task Force Data Base pilot program • Resources to scale the infrastructure into the Beacon region • Will pilot first in targeted schools and use lessons learned to generalize the technology approach • Widespread implementation of a technology solution will take time • Strong emphasis on protecting the confidentiality and best interests of patients • Multiple EHRs 45
Qualitative Study / Focus Groups • Groups of interest: • Parents of school aged children w/ asthma • School nurses & others that care for children with asthma in schools • School aged adolescents with asthma • Physicians / nurses who provide health care for children with asthma Identify perceived needs and potential barriers related to the wide spread use of asthma action plans for school children. 46
Focus Group Analysis:Overarching Themes Communication Stakeholders Pairings – parent/school, school/health professional, school/health professional Channels Fax, flyers, walkie talkies, computer interface, paper copies, telephone Frequency and timeliness Asthma severity and control Continuum Individual Self-reliance Support for students’ independence Awareness of potential triggers 47
Focus Group Analysis:Overarching Themes • Policies and Protocol • Confidentiality • Initiating processes – i.e. updating AAPs • Education of staff • “What are we allowed to do” • Assurance of medication in secondary settings (i.e. field trips, sporting events) • Alignment with state laws, school policies and “unwritten rules” of communication 48
Survey Results:Nurses and Physicians AAPs are an important tool for schools and families It is important to evaluate whether AAPs make a difference in the care of asthma in schools It would be helpful to the care of patients with asthma to have communications with schools (missed PE, sent home, child’s technique and understanding of disease) 90% agree with the concept that consistency in adhering to guidelines is needed Time to create the AAP is a constraint for physicians and nurse practitioners (80% no more than 3 minutes of time – preference to review, not create) Would like to know more about how the AAP is used at school and the training within the schools of those with access to the AAP 49
Focus Groups-School Sites(School Nurse, Health office, Teachers & Coaches) • Knowing what to do with Student is Important • Asthma Action Plans are useful to Health Office staff • Coaches rely on 1st Aid Training to know what to do • Issues • Inhalers are kept in Health Office • Communication of Changes in med order or plan • Suggestions • Access to electronic information would help 50