Download
1 / 24
240 likes | 249 Views
secondary prevention, prior MI, stents, aggressive, male, 67-year-old)

E N D
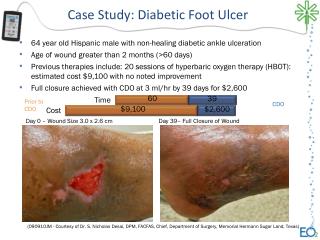
67 Year Old Male with Prior MI (stents x6) Interested in Aggressive Secondary Prevention Case Category: Secondary Prevention History of present illness: 67 year old male with prior MI and stents. Interested in secondary prevention.
Labs on Pravachol 80, Niaspan 1000 This is an older NMR report which previously did not report an IR-Score (Insulin resistance score). Current reports will give an IR-Score and if >45 suggests insulin resistance present. We would suspect in this case it would be in normal range. Here we see no evidence of insulin resistance as a secondary cause of Dyslipidemia. Niaspan improves markers of insulin resistance so may also be normal as he is on this therapy.
NMR LipoProfile • Insert NMR LipoProfile 07312009 TU41 Insert
Questions to Consider • Question 1: He is on low dose Niaspan. How well is he tolerating? Better tolerated if taken after a meal preceded by 325 mg uncoated aspirin if no contraindications. Also can try psyllium supplement with meal or applesauce to help reduce Niaspan side effects. Avoid alcohol, hot beverages. If flushing occurs chew a few 81 mg baby aspirin to help stop flush. • Question 2: Any prior history of elevated glucose? HgAIC 5.9 currently which is in borderline zone (5.7-6.4). In the setting of Niaspan use may be increased slightly as glucose may transiently increase. NO evidence of insulin resistance on NMR so would treat with diet (low carb) and exercise but not necessarily treat with Metformin as this may just be Niaspan effect not impacting beta cell function. Following closely is the key.
Questions to Consider • Question 3: How much omega 3 is he really taking? Cardiovascular benefit if EPA/DHA is 1 gram or more. Look at the fish oil bottle and review amount of EPA/DHA in the serving size. Most patients are taking much lower dose than the front of the bottle reflects. For triglyceride reduction they will need at least 3-4 grams EPA/DHA. In his case only low dose needed. He reports higher doses have caused “fishy burp”. • Question 4: Flax seed has benefit but the oil is less beneficial than the seeds. Only about 10 % of ALA will convert to omega 3. We advise if using flax to use real flax seeds not the oil, keep small amount in refrigerator to keep it fresh, grind in a coffee grinder right before use and add to food, cereal, yogurt etc.
Initial Treatment & Management • Stop Pravachol 80 mg • Start Crestor 20 mg/day • Start Lovaza 1 g/day • Increase Niacin from 1000 to 2000 mg/day • Continue CO Q 10 supplement • Start Vitamin D3 3000-4000 IU/daily
Follow Up • CAD – Asymptomatic on Plavix. • Familial Combined Hyperlipidemia – Improved on Crestor 20 mg, Niacin 2000 mg and Lovaza 1 g/day; LDL-P reduced from 1004 to 466; LDL-C down to 58 from 107; Continue therapy. • Elevated Lp(a) – Unchanged; On Niacin 2000 mg/day; Continue therapy. • Elevated LpPLA2 – Improved with slight decrease from 212 to 207; Continue therapy, consider higher dose omega 3. Increase lovaza from 1-2/day. • Vitamin D Deficiency/Fatigue – Improved with 3000-4000 IU/day Vitamin D3 gel caps from 30 to 43; Continue therapy. • Diet - Reduce carbs, elevation in small dense LDL may be due to high carb diet.
Apo E genetic testing Apo E4E4 genotype suggests he is genetically at higher cardiovascular risk but also may not respond well to high dose statin therapy. At this point we are using combination therapy which is appropriate. Previous studies suggest high dose statins are not effective when E4 mutation present and we do see these patients respond less well to medication.
Clinical Pearls Elevated Lipoprotein (a) is an important marker of increased genetic risk for cardiovascular disease especially in the setting of premature disease or family history of premature cardiovascular disease. There are many issues with the lipoprotein(a) assay. Important to note this patient had 2 different Lp(a) assays, one nmol/L assay with a reference range <75 normal and one with mg/dl assay with a reference range <30 mg/dL. The 2 values cannot be compared. It is high regardless. Small studies have also shown benefit with high dose omega 3 fatty acids. See comments under lipoprotein (a) under the clinical treatment index elsewhere on this site.
References • Brunzell JD, Davidson M, Furberg CD, et al. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008 Apr;31(4):811-22. • Nicholls SJ, Ballantyne CM, Barter PJ, et al. Effect of two intensive statin regimens on progression of coronary disease. N Engl J Med 2011; DOI: 10.1056/NEJMoa1110874. • Rosenson, RS and Hsia Otvos. Effects of rosuvastatin and atovastatin on LDL and HDL particle concentrations in patients with metabolic syndrome: a randomized, double-blind, controlled study. Diabetes Care. 2009 Jun;32(6):1087-91. • GISSI-P Investigators. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzion trial. Lancet. 1999;354(9177):447-455. • ContoisJH, McConnell JP, Sethii AA, et al. Apolipoprotein B and cardiovascular disease risk: position statement from the AACC Lipoproteins and Vascular Diseases Division Working Group on Best Practices. ClinChem2009 Mar;55(3):407-19. • Ballantyne C, Herd JA, Stein E, et al. Apolipoprotein E genotypes and response of plasma lipids and progression-regression of coronary atherosclerosis to lipid-lowering drug therapy. J Am CollCardiol2000;36:1572-8. • Roth EM, Bays HE, Forker AD, et al. Prescription omega-3 fatty acid as an adjunct to fenofibrate therapy in hypertriglyceridemic subjects. J CardiovascPharmacol. Jul 10 2009;