Download
1 / 35
350 likes | 767 Views
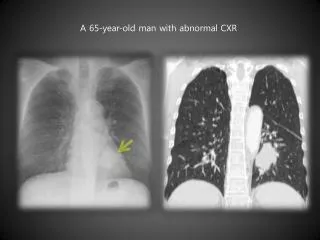
67 Year Old Woman with an Abnormal Chest CT. Andrea Glassberg March 11, 2003. Clinical Presentation. A 67 year old woman with a history of breast cancer and mediastinal mass presented to chest clinic with an abnormal CT scan of the chest.

E N D
67 Year Old Woman with an Abnormal Chest CT Andrea Glassberg March 11, 2003
Clinical Presentation A 67 year old woman with a history of breast cancer and mediastinal mass presented to chest clinic with an abnormal CT scan of the chest. She reported three months of progressive dyspnea on exertion and dry cough without chest pain or wheezing.
Past Medical History • Breast Cancer (1991), S/P lumpectomy, XRT • Mediastinal Mass (1999), initially believed to be metastatic disease • DM II • HTN
Medications • Losartan • Glucophage • Glyburide • Clonidine • HCTZ • Nifedipine • Celebrex • Prinomastat (metalloprotease inhibitor)
Exam • Obese, tired appearing AA woman • Afebrile • 150/85 • HR 125 • RR 22 • O2 sat 91% on RA • Coarse inspiratory crackles • No peripheral edema
PFT 9-8-02 • VITAL CAPACITY 1.9 LITERS 71 % • EXPIRATORY RESERVE VOL 0.2 LITERS 33 % • TLC BY SINGLE BREATH 2.9 LITERS 56 % • TLC BY HE RE-BREATHING 3.6 LITERS 81 % • DIFFUSING CAP, HGB COR 15.1 59 % • DIF. CAP. HGB COR/TLC 5.2 102 % • FORCED VITAL CAPACITY 2.0 LITERS 74 % • FORCED EXPIRED VOL 1 S 1.6 LITERS 77 % • % EXPIRED 1 SECOND 81 % 106 % • FEF 25-75% 1.6 L/SEC 73 % • FEF 25% 3.8 L/SEC 72 % • FEF 50% 2.2 L/SEC 50 % • FEF 75% 0.6 L/SEC 28 %
BAL • Hazy • 405 RBC • 395 WBC • 16% N • 34% L • 43% M/H/M • 6% Eos • Cx neg
Transbronchial Biopsy The biopsy shows numerous polypoid plugs of granulation tissue within the airspaces, type II cell hyperplasia, and a sparse interstitial lymphocytic infiltrate.
Interval History The patient was started on Prednisone, 60 qd and had almost complete resolution of her symptoms within two weeks. However, she subsequently developed severe side effects from prednisone, including candida esophagitis, and difficult to control hyperglycemia.
PFT 11-12-02 • TLC BY SINGLE BREATH 3.2 LITERS 62 % • DIF. CAP. HGB UNCOR. 15.4 61 % • DIF CAP HGB UNCOR/TLC 4.8 94 % • FORCED VITAL CAPACITY 1.8 LITERS 69 % • FORCED EXPIRED VOL 1 S 1.5 LITERS 75 % • % EXPIRED 1 SECOND 84 % 110 % • FEF 25-75% 1.8 L/SEC 83 % • FEF 25% 4.3 L/SEC 80 % • FEF 50% 2.5 L/SEC 56 % • FEF 75% 0.7 L/SEC 34 % • PO2 ARTERIAL BLOOD GAS 124 MMHG • PCO2 ARTERIAL BL. GAS 32 MMHG • PH, ARTERIAL BLOOD GAS 7.48
Interval History The dose of prednisone was tapered from 60mg qd to 20mg qd over 4 months. The patient then self d/c’d the medication.
PFT 2-18-03 • VITAL CAPACITY 2.3 LITERS 86 % • TLC BY SINGLE BREATH 3.2 LITERS 60 % • TOTAL LUNG CAP. (BOX) 3.8 LITERS 86 % • TLC BY HE RE-BREATHING 3.9 LITERS 87 % • DIFFUSING CAP, HGB COR 17.0 67 % • DIF. CAP. HGB UNCOR. 15.2 60 % • DIF. CAP. HGB COR/TLC 5.4 107 % • FORCED VITAL CAPACITY 2.3 LITERS 87 % • FORCED EXPIRED VOL 1 S 1.8 LITERS 89 % • % EXPIRED 1 SECOND 79 % 104 % • FEF 25-75% 1.7 L/SEC 80 % • FEF 25% 4.9 L/SEC 92 % • FEF 50% 2.5 L/SEC 55 % • FEF 75% 0.5 L/SEC 25 % • AIRWAY RESISTANCE 4.2 CMH2O/LPS
COP Cryptogenic Organizing Pneumonitis
Idiopathic (COP) Rapidly Progressive Focal Nodular Postinfection Drug Related Rheumatologic/CTD Immunologic Organ Transplantation Radiotherapy Environmental Exposures Miscellaneous IBD Lymphoma and cancer HIV MDS Hunner Interstitial Cystitis Chronic thyroiditis and ETOH cirrhosis Seasonal syndrome with cholestasis PBC CABG Classification of BOOP
BOOP Syndrome • Radiation therapy to the breast within 12 months, 2) General and/or respiratory symptoms lasting for at least 2 weeks, • Radiographic lung infiltrates outside the radiation port 4) No evidence of a specific cause
Epidemiology of COP • Six to seven per 100,000 hospital admissions was found at a major teaching hospital. • Onset typically in the fifth or sixth decades. • Both genders affected equally. • Short duration of symptoms (<3 mo). • Cigarette smoking is not a precipitating factor.
Duration of Symptoms King, Cryptogenic Organizing Pneumonia. UpToDate online 11.1
Clinical Findings • Often mimics CAP • Fever • Malaise • Fatigue • Cough • Persistent nonproductive cough • Dyspnea with exertion • Weight loss of greater than 10 pounds (57 %) • Inspiratory rales (74%) • Normal lung exam (25%)
Imaging • Bilateral, diffuse alveolar opacities in the presence of normal lung volumes. • A peripheral distribution of the opacities, similar to that seen in chronic eosinophilic pneumonia. • Recurrent or migratory pulmonary opacities (up to 50 %). • Irregular linear or nodular interstitial infiltrates rarely the only radiographic manifestation. • Honeycombing rare, occurs as a late manifestation in patients with progressive disease. • Rare features: • pleural effusion • pleural thickening • Hyperinflation • cavities
Physiology • Moderate restrictive disorder • Diffusion abnormality • Resting hypoxemia common • Obstruction rare
King, Cryptogenic Organizing Pneumonia. UpToDate online 11.1
King, Cryptogenic Organizing Pneumonia. UpToDate online 11.1
King, Cryptogenic Organizing Pneumonia. UpToDate online 11.1
Treatment • Prednisone 1-1.5mg/kg for 6-8 weeks. • Taper slowly over a period of 6 months to 1 year. • Cyclophosphamide as a steroid sparing agent.
Outcome King, Cryptogenic Organizing Pneumonia. UpToDate online 11.1
Relapses Am J Respir Crit Care Med Vol 162. pp 571–577, 2000
Relapses Am J Respir Crit Care Med Vol 162. pp 571–577, 2000
Relapses Am J Respir Crit Care Med Vol 162. pp 571–577, 2000
COP Pearls • Diagnosis of exclusion (BOOP w/o cause) • Histologic appearance is granulomatous infiltration of distal airspaces • Lung architecture is preserved • Responsive to steroids • Relapses common • No need to treat to prevent relapses
References • Crestani, et al., Bronchiolitis Obliterans Organizing Pneumonia Syndrome Primed by Radiation Therapy to the Breast. Am J Respir Crit Care Med (1998)158:1929–1935. • Epler, Bronchiolitis Obliterans Organizing Pneumonia. Arch Intern Med. (2001) 161:158-164. • King, Cryptogenic Organizing Pneumonia. UpToDate online 11.1. • Lazor, et al., Cryptogenic Organizing Pneumonia, Characteristics of Relapses in a Series of 48 Patients, Am J Respir Crit Care Med (2000) 162: 571–577. • Mokhtari, et al., Bronchiolitis obliterans organizing pneumonia in cancer: a case series. Respiratory Medicine, (2002) 96: 280-286. • Oikonomou and Hansell, Organizing pneumonia: the many morphological faces. Eur Radiol (2002) 12:1486–1496. • Takigawa, et al., Bronchiolitis Obliterans Organizing Pneumonia Syndrome In Breast-conserving Therapy For Early Breast Cancer: Radiation-induced Lung Toxicity. Int. J. Radiation Oncology Biol. Phys. (2000) 48: 751–755.