Download
1 / 17
170 likes | 256 Views
Innovative peer-to-peer educational intervention to reduce HIV and other blood-borne infection risks in difficult–to-reach people who inject drugs: results from the ANRS AERLI study.

E N D
Innovative peer-to-peer educational intervention to reduce HIV and other blood-borne infection risks in difficult–to-reach people who inject drugs: results from the ANRS AERLI study Patrizia Carrieri, Jean-Marie Le Gall, Marie Debrus, Baptiste Demoulin, Caroline Lions, Aurélie Haas, Marion Mora, Perrine Roux, Marie Suzan-Monti, Bruno Spire
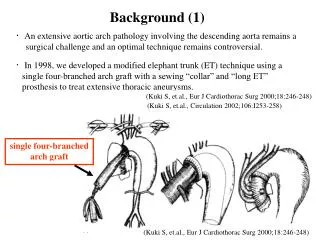
Background (1) • French harm reduction policies havecontributed to vastly reduceHIV incidence among people who inject drugs (PWID) • ~1% of new HIV diagnoses in 2012 • However, complications related to injecting practices remain • High prevalence of Hepatitis C Virus (HepC) infections • Needle/syringe and paraphernalia sharing • Other intravenous drug use related complications • Local lesions : venous damage, abscesses, cellulitis, other skin infections • Cardiovascular and pulmonary complications
Background (2) • Existence of persisting at-risk behaviors suggests that current Harm Reduction Programs are insufficientfor PWID • Opiate substitution treatments • Needle/syringe programs • Support services • Need to experiment with, evaluate and implement alternative and innovative strategies that effectively improve the health of this population
Objective • The objective was to assess the effectiveness and feasibility of a community-based training and education intervention on reducing injection-associated risks • Viral infections (HIV, HepC) • Other injection-related damages • AIDES and Médecins du Monde staff members or volunteers were involved in study design, training of peers, performing the intervention, collecting and analyzing the data
Study design (1) • National multi-site community-based study comparing the evolution of injection- related risks over one year in low-threshold services, hold by AIDES and MDM, between: • An intervention group, comprising people benefitting from educational sessions in 8 participating services • A control group, comprising people recruited in 9 services, working in accordance with current guidelines
Study design (2) Educational sessions (ES) with PWID = educational tailored intervention by NGO staff member/volunteer after observation of participants’ self-injection practices Phone interviews with an independent trained interviewer not involved in the ES At least1 ES over 5 months Intervention group Control group Inclusion M6 M12
Methods (1) • Eligibility criteria • ≥18 years old; injecteddrug at least once during the previous week; willing to be contacted for a phone interview; able to provide written informed consent • Data collection • Phone interviews at M0, M6 and M12 collecting : • socio-demographic characteristics • behaviors related to HepC transmission risk (BBV-TRAQ) • experience with drug use; history of incarceration • access to care; HIV, Hep C and B testing and diagnosis • motivational factors for willing to participate in the intervention • Data from the intervention sessions were collected by community-based association members
Methods (2) • Analyses • Outcomes • Having at least one at-risk practice for HepC transmission in the previous month • Having at least one local complication at the injection site • 2-step Heckman model to avoid possible selection bias arising from the clustering of intervention (n=113) and control groups (n=127) • 1st step: probit model to identify baseline factors associated with exposure to the ES to compute the inverse Mills ratio (IMR) • 2nd step: probit mixed model to identify factors associated with each outcome after introducing the IMR to control for the clustering bias
Study sample diagram Control sites n=9 Intervention sites n=8 Participants who did not receive ES N=31 288 ES
Results (1) – Participants’ characteristics Baseline characteristics (n (%) ormedian [IQR]), ANRS-AERLI study (n=240) † Chi-squared test or Wilcoxon test § in years ⱡ AUDIT score ≥3 for women; ≥4 for men *during the previous 4 weeks 1more than 1 HCV at-risk practice during the previous month 2more than 1 problem at the injection site
Results (2) – Evolution of the outcomes • Percentage of participants who reported at least one complication at the injection site • Percentage of participants who reported at least one HCV at-risk practice • p<0.05 : significant difference between M0 and M6 • in the intervention group • p<0.05 : significant difference between M0 and M12 • in the intervention group
Results (3) - Impact of education intervention on HCV risk practices Multivariate model (n = 238, visits = 497)
Results (4) - Impact of education intervention on local complications at the injection site Multivariate model (n=240, visits=520)
Discussion • Limitations • Difficult to have a comparable control group because of clustering • High diversity of PWID population • Lost to follow-up • Self-reports • Positive impact of this innovative education intervention on injecting practices in terms of • A decrease in HCV at-risk practices • A reduction in local complications at the injection site
Conclusion • Innovative aspects of this intervention • Peer-based intervention • Short intervention • Low-cost intervention • Intervention that may be used in several contexts • Needle/syringe programs, safer injecting facilities, outreach intervention in settings where prevalence of PWID is high
Acknowledgements • People who agreed to participate in the study • The ANRS-AERLI study group : M. Beaumont ; G. Boyault ; P.M. Carrrieri ; M. Debrus ; A. Haas ;J.M. Legall; G. Maradan ; M. Mora ; M. Préau ; P. Roux : B. Spire ; M. Suzan-Monti • All participating centers and their staff: M. Debrus (Paris); G. Boyault (Nevers); G. Penavayre (Pau); C. Labbé (Lille); C. Urdiales (Nîmes /Alès); J. Murat (Toulouse); C. Saramago (Grenoble); F. Tempez (Rennes); N. Perrin (Clermont Ferrand); G. Dubosc (Avignon); N. Rodier (Limoges); M. Louanges (La Roche sur Yon); F. Rigaud (Béziers); M. Alvès Da Costa (Nancy) • Funding