Download
1 / 14
140 likes | 345 Views
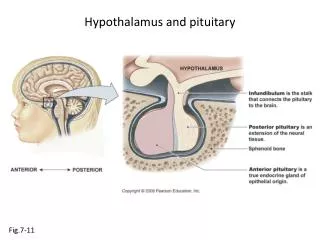
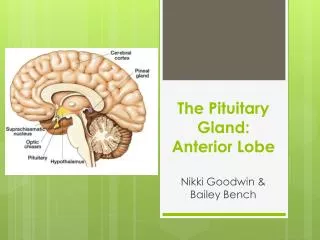
Hypothalamus and the anterior pituitary. The Hypothalamus pituitary axis synthesize. Hypothalamus, TRH , CRH Ant. PIT. Produce : ACTH TSH FSH LH G.H Post.Pitu. produce : ADH Oxytocin. Control: Through Hypothalamic releasing , inhibitor factors Stress . Hypoglycaemia.

E N D
The Hypothalamus pituitary axis synthesize • Hypothalamus, TRH , CRH Ant. PIT. Produce : • ACTH • TSH • FSH • LH • G.H Post.Pitu. produce : ADH Oxytocin
Control: Through Hypothalamic releasing , inhibitor factors • Stress . • Hypoglycaemia. Disorders of Anti- pitruitary Hormones secretion :
Excess Def. ACTH Cushing (rare) Hypoadrenalism TSH Hyperthyroidism 2nd hypothyroidism LH/FSH early puberty 2nd hypogonaidism infertility Excess GH: Gigantism. Acromegaly. Excessive hair growth. Compression of the optic chiasma may cause visual field defects.
Diagnosis of the hypothalamic pituitary axis disorders : • Clinical presentation . • Radiological findings. • Plasma GH is increased. • Raised plasma glucose. • Diganosis is confirmed by: • Demonstrating Raised plasma GH not suppressed by a rise in plasma glucose concentration. • In normal subjects plasma GH falls to low levels.
hypopituitarism Causes: • Destruction or damage to the gland by tumour • Infarction :post partum haemorrhage (Sheehan’s syndrome) • Pituitary surgery or irradiation. • Head injury or granuloma.
Effects: • Secondary hypogonadism presenting as :amenorrhea, infertility , atrophy of secondary sexual characteristics. • Growth retardation in children . • Secondary hypothyroidism. • Secondary hypoadrenalism and hyperpigmentation . • Prolactin deficiency with failure to lactate .
Adrenal disorders Adrenal hormones and their effects : • Cortisol controlled by ACTH through –ve feed back mechanism . • Stress . Effects : • CHO metabolism disorder causing hyperglycemia since it is hyperglycemic hormone. • Aldosterone controlled by rennin - angiotensin system. • Effects: reabsorption of Na and excretion of K
Disorders of adrenal cortex1 Cushing ‘s syndrome: Due to excessive cortisol and ACTH. Effects: Obesity. Impaired glucose intolerance. Increased protein catabolism. Hypertension. Psychiatric disturbances.
Causes of Cushing’s syndrome : 1.Adrenal hyperplasia : • Morning and evening plasma cortisol raised. and not suppressed by dexamethasone. • ACTH level is very law . 2.Ectopic ACTH : • Plasma cortisol raised day and evening. • Plasma ACTH is high. • Not suppressed even after 8 mg dexamethasone.
Investigation of suspected cushing’s syndrome: • Plasma cortisol morning raised . • Plasma cortisol evening raised . • Urinary free cortisol raised . • After 2mg dexamethasone no suppression .
Adrenocortical hypofunction Addison’ disease : • Caused by: 1.Bilateral destruction of all zones of the adrenal cortex because of auto immune process. 2.T.B 3. Amyloid. 4. secondary deposit. 5.Haemorrhage into adrenal glands following meningitis.
Clinical presentation : • Acute hypo function :adrenal crisis . • Shock • Features due to hyponatraemia and hyperkalaemia . • Hypoglycemia • Androgen deficiency . • Pigmentation.