Download
1 / 16
180 likes | 762 Views
Ultra-High Resolution Optical Coherence Tomography in the Diagnosis of Conjunctival /Corneal Intraepithelial Neoplasia and Pterygia. Jeremy Z. Kieval , MD; Rodrigo A. Hoffman, MD; Sander R. Dubovy , MD; Mohamed A. Shousha , MD, PhD; Jianhua Wang, MD, PhD; Carol L. Karp, MD

E N D
Ultra-High Resolution Optical Coherence Tomography in the Diagnosis of Conjunctival/Corneal Intraepithelial Neoplasia and Pterygia Jeremy Z. Kieval, MD; Rodrigo A. Hoffman, MD; Sander R. Dubovy, MD; Mohamed A. Shousha, MD, PhD; Jianhua Wang, MD, PhD; Carol L. Karp, MD Bascom Palmer Eye Institute, University of Miami, Miami, Florida The authors have no financial interest in the subject matter of this poster
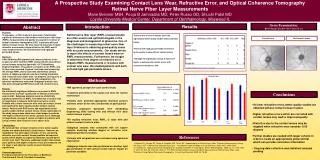
Abstract • Purpose: To assess the use of ultra-high resolution optical coherence tomography (UHR-OCT) in distinguishing conjunctiva/corneal intraepithelial neoplasia (CIN) and pterygia, and compare this with histopathologic specimens. • Methods: 34 eyes with conjunctival/corneal lesions suspicious for CIN or pterygia were imaged with a custom built UHR-OCT. Each patient underwent excisional or incisional biopsy with histopathological diagnosis of the lesion. UHR-OCT images were compared with histopathologic specimens to determine the correlation between histology and UHR-OCT images. Epithelial thickness of all UHR-OCT images was measured and differences were examined using a Student’s t-test. • Results: UHR-OCT images of CIN demonstrated striking similarities to histopathologic specimens. Both optical and pathological specimens showed a thickened, disorganized layer of epithelium. Likewise, UHR-OCT images of patients with pterygia were well correlated with histopathologic specimens showing a normal epithelium, with underlying thickening and hyperreflectivity of the subepithelial mucosal layers. Differences in epithelial thickness between CIN and pterygia were statistically significant with a mean epithelial thickness of 355 μm (sd=170) in CIN patients and 100 μm (sd=22) in pterygium patients (p<0.001). • Conclusions: UHR-OCT may be a promising diagnostic tool for a non-invasive evaluation of ocular surface lesions, including CIN and pterygia.
Introduction • The term conjunctival intraepithelial neoplasia (CIN) was first coined in 1978 by Pizzarello and Jacobiac.1 CIN can involve the conjunctiva, the cornea, or both. This spectrum of disease is often referred to as ocular surface squamousneoplasia (OSSN). The diagnosis can be made clinically by identification of the characteristic appearance of an elevated, gelatinous, papilliform, or leukoplakic lesion, often accompanied by a feeder vessel and demonstrating positive Rose-Bengal staining. However, these lesions can sometimes present in the absence of such “textbook” findings, and can sometimes be difficult to distinguish between other ocular surface lesions. • The “gold-standard” for diagnosis of OSSN is histopathological specimen by incisional or excisional biopsy. Clinical diagnosis can also be confirmed by brush cytology and impression cytology.2-6 • Anterior segment optical coherence tomography (AS-OCT) has the potential to provide a non-invasive, optical biopsy of tissue, where morphologic and even histologic characteristics can be examined in vivo. The recent introduction of AS-OCT has enabled assessment of the conjunctiva and cornea with high axial resolution of tissue planes.7 Time-domain technology achieves an axial resolution of approximately 18 µm. However, using Fourier (spectral) domain signal analysis, the axial resolution of images can be improved to near 8 µm in commercially available units. New custom-built ultra-high resolution units have allowed axial resolution of 2-3 µm, and have been shown to enable morphologic visualization of both corneal and retinal architecture.8 • The aim of the present study was to assess the use of an ultra-high resolution optical coherence tomography (UHR-OCT) as an adjuvant tool in diagnosing CIN and pterygia when compared with histopathologic tissue biopsy.
Methods • This study was approved by the University of Miami Institutional Review Board (IRB) committee, and was conducted in accordance with the principles of the Declaration of Helsinki. Written, informed consent was obtained from all study participants. Patients • A retrospective review of 34 eyes of 33 patients seen at one institution (Bascom Palmer Eye Institute) was performed for the present study. All patients were imaged using a custom built UHR-OCT. Radial, 12mm images of the appropriate region were acquired at a rate of 32 frames/scan to capture the conjunctival/corneal lesions. Obtained histopathologic specimens of the remaining 34 eyes were then reviewed for data collection, and the findings were correlated with the pre-operative UHR-OCT images. Spectral domain optical coherence tomography • A custom built, high speed and ultra-high resolution spectral domain optical coherence tomography was used for this study. This device uses a three-module superluminescent diode (SLD) light source (Broadlighter, T840-HP, Superlumdiodes Ltd, Moscow Russia) with a center wavelength of 840nm and a full width at half maximum bandwidth of 100 nm. The calibrated axial resolution of the system was ~4 µm in the air and ~3 µm in water or tissue (the refractive index is ~1.39). Statistical Analysis: • SPSS software version 17.0 (SPSS, Chicago, IL, USA) was used for statistical analysis. Means of age and measured epithelial thicknesses of the lesions and the adjacent unaffected cornea were compared between the CIN and the pterygium groups with a two-sided Student t-test. P-values less than 0.05 were considered statistically significant. Values are presented as means ± standard deviation. Categorical variables, such as gender, were compared with the chi-square test. Sensitivity and specificity of epithelial thickness for both groups of subjects are presented to evaluate this measurement as a diagnostic tool.
Results • Seventeen eyes had conjunctival and/or corneal lesions that disclosed a ocular surface neoplasia. • Histopathologic specimens in all patients with CIN demonstrated conjunctival and/or corneal epithelium with faulty maturational sequencing extending either partial or full thickness. All patients showed acanthotic epithelium often with variable degrees of chronic inflammatory cell infiltrates in the substantiapropria. An abrupt transition from normal to abnormal epithelium could be demonstrated in obtained pathological specimens. • UHR-OCT images of all OSSN lesions were captured and showed a severely thickened, hyper-reflective epithelium. In most cases, an abrupt transition between the normal and the affected thickened epithelium was evident. Images were remarkably similar to the histopathological specimens (Figures 1, 2, and 3). • Seventeen eyes of 16 patients underwent histopathological biopsy of conjunctival and/or corneal lesions that disclosed a pterygium. • Histopathologic specimens in all patients with pterygia demonstrated a normal conjunctival epithelium without acanthosis. Mild to moderate degrees of actinic change were seen in the underlying substantiapropria. • UHR-OCT images of all pterygia were captured and showed a normal thin epithelial architecture, and reflectivity. The underlying subepithelial tissue showed hyper-reflectivity. These findings were also very similar to the corresponding histopathologic specimens, as demonstrated in figures 4, 5, and 6.
Results • Statistical analysis between the two groups is seen in Table 1. • A statistically significant difference in age between groups was seen with a mean of 70.5 years of age (sd=14) in CIN patients, and 41 years of age (sd=16) in pterygia patients (p<0.001). • The difference in epithelial thickness between CIN patients and pterygia patients was statistically significant. The mean epithelial thickness was 355m (sd=170) in CIN patients and 100m (sd=22) in pterygium patients (p<0.001, t-test). • Epithelial thickness in non-tumor areas was also measured in each patient, and there was no significant difference between the mean of 93m (sd=48) in CIN patients, and a mean of 73m (sd=12) in pterygium patients (p=0.11). • Receiver operating characteristic (ROC) curves show that there is hardly any overlap between the two groups. The area under the ROC curve is 94%. The CIN range of epithelial thickness was 68 to 740m and for pterygia, the range was 69 to 136m. • Using 150m as a cutoff, UHR-OCT has a sensitivity of 94% and specificity of 100%.
Table 1 * Student t-test ** Chi-square test
Conclusions • Conjunctival/corneal intraepithelial neoplasia is the most common non-pigmented ocular surface neoplasm.9,10 Surgical treatment consists of wide local excision with adjunctive cryotherapy to the surgical margins in a double-freeze-thaw technique. Incomplete excision is common due to diffuse lateral growth, and is associated with a higher incidence of recurrence after surgery.11 Despite clear surgical margins, recurrence of neoplasia can range from 5% to 33%.11,12 • Recent advances in topical chemotherapeutic agents have become a valuable alternative in the non-invasive management of CIN. They can be used as primary treatment, adjuvant therapy to surgery, or treatment of recurrent neoplasia. The principal agents that are used include mitomycin-C (MMC)12-17, 5-fluorouracil (5-FU)18-20, and interferon alpha 2β (INFα 2β).21-23 • With the advantages of medical therapy for CIN, it would be certainly be ideal in such situations to have a method of examining the anterior segment structures with microscopic detail to help guide and tailor such medical treatment. • The results of our study have demonstrated a compelling correlation between images obtained by UHR-OCT and histopathology in patients with CIN and likewise, in cases of pterygia. With resolution matching that of histologic specimens, UHR-OCT was able to provide a clear diagnosis of CIN using minimally invasive technology. The applications of these results are significant. The use of a minimally invasive diagnostic tool can potentially preclude the need for tissue biopsy causing conjunctivalcicitrization and patient discomfort. This is especially important in an era of increasing use of topical chemotherapeutic agents that obviate the need for surgical excision and cyrotherapy. • In addition to the potential use of UHR-OCT for diagnosis, patient follow-up during the course of medical treatment and continued surveillance for neoplasia may be possible without the need for repeated biopsies. It may also be helpful in detecting early recurrent disease, or if a surgical excision is planned, the OCT may be helpful in determining the extent of disease to facilitate complete excision. • In conclusion, UHR-OCT appears to be a promising technology for a non-invasive diagnosis and surveillance of patients with CIN. While UHR-OCT is not a substitute for histopathological specimens, it does appear to be a valuable diagnostic adjuvant in the clinical diagnosis of anterior segment pathology. It may also provide a non-invasive manner to monitor for recurrence after surgical excision or medical treatment. The high axial resolution provided in cross sectional images demonstrates an excellent correlation to cellular features in histopathological specimens. Further studies are necessary to determine the sensitivity and specificity of UHR-OCT in identifying ocular pathology.
References • Pizzarello LD, Jakobiac FA. Bowen’s disease of the conjunctiva: a misnomer. In: Jakobiac FA ed. Ocular and Adnexal Tumors. Birmingham, AL: Aesculapius; 1978:553-571. • Gelender H, Forster RK. Papanicolaou cytology in the diagnosis and management of external ocular tumors. Arch Ophthalmol 1980; 98:909-912. • Tsubota K, Kajiwara K, Ugajun S, et al. Conjunctival brush cytology. Acta Cytol 1990; 34: 233-235. • Tseng SCG. Staging of conjunctival squamous metaplasia by impression cytology. Ophthalmol 1985; 92:728-733. • Nolan GR, Hirst LW, Wright RG, et al. Application of impression cytology to the diagnosis of conjunctival neoplasms. Diagn Cytopathol 1994; 11:246-249. • Tole D, MecKelvie P, Daniell M. Reliability of impression cytology for the diagnosis of ocular surface squamous neoplasia employing the Biopore membrane. Br J Ophthalmol 2001; 85:154-158. • Izatt JA, Hee MR, Swanson EA, et al. Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Arch Ophthalmol 1994; 112:1584–1589. • Drexler W, Morgner U, Ghanta RK, et al. Ultrahigh-resolution ophthalmic optical coherence tomography. Nat Med 2001; 7:502–507. • Grossniklaus HE, Green WR, et al. Conjunctival lesions in adults: a clinical and histopathological review. Cornea 1987; 6:78-116. • Shields, CL and Shields, JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol 2004; 49:3-24. • Tabin G, Levin S, Snibson G et al. Late recurrences and the necessity for long term follow up in corneal and conjunctival Intraepithelial Neoplasia. Ophthalmol 1997; 104:485-92. • Frucht-Pery J, Sugar J, Baum J, et al. Mitomycin C treatment for conjunctival-corneal intraepithelial neoplasia: a multicenter experience. Ophthalmol 1997; 104:2085-93. • Kemp EG, Harnett AN, Chatterjee S. Preoperative topical and intraoperative local mitomycin C adjuvant therapy in the management of ocular surface neoplasias. Br J Ophthalmol 2002; 86:31-34. • Heigle TJ, Stulting RD, Palay DA. Treatment of recurrent conjunctival epithelial neoplasia with topical mitomycin C. Am J Ophthalmol 1997; 124:397-99 • Haas K, Ben-Dor D, Levartovsky S. Treatment of conjunctival corneal intraepithelial neoplasia with topical mitomycin C. Arch Ophthalmol 1999; 117:544-45. • Shields CL, Naseripour M, Shields JA. Topical mitomycin C for extensive, recurrent conjunctival-corneal squamous cell carcinoma. Am J Ophthalmol 2002; 133:601-6. • Singh G, Wilson MR, Foster CS. Long-term follow-up study of mitomycin eye drops as adjunctive treatment for pterygia and its comparison with conjunctival autograft transplantation. Cornea. 1990; 9:331-34.
References • Yeatts RP, Ford JG, Stanton CA, et al. Topical 5-fluorouracil in treating epithelial neoplasia of the conjunctiva and cornea. Ophthalmol 1995; 102:1338-44. • Midena E, Boccato P, Angeli CD. Conjunctival squamous cell carcinoma treated with topical 5-fluorouracil. Arch Ophthalmol 1997; 115:1600-01. • Yeatts RP, Engelbrecht NE, Curry CD, et al. 5-Fluorouracil for the treatment of intraepithelial neoplasia of the conjunctiva and cornea. Ophthalmol 2000; 107:2190-95. • Vann RR, Karp CL. Perilesional and topical interferon alfa-2b for conjunctival and corneal neoplasia. Ophthalmol 1999; 106: 91-7. • Karp CL, Moore JK, Rosa RH. Treatment of conjunctival and corneal intraepithelial neoplasia with topican interferon alpha-2b. Ophthalmol 2001; 108: 1093-8. • Schechter BA, Koreishi AF, Karp CL, et al. Long-term follow-up of conjunctival and corneal intraepithelial neoplasia treated with topical interferon alfa-2b. Ophthalmol 2008; 115:1291-6.