Download
1 / 22
220 likes | 324 Views
Explore TDF resistance risk in a tenofovir prophylaxis trial in Botswana through a mathematical model, assessing the impact on participants and potential mitigation strategies.

E N D
Antiretroviral resistance is not an important risk of the oral tenofovir prophylaxis trial in Botswana: a simple mathematical modeling approach Dawn K. Smith, Poloko Kebaabetswe, Kisanga Disasi, Douglas Fleming, Lynn Paxton, and Margarett Davis
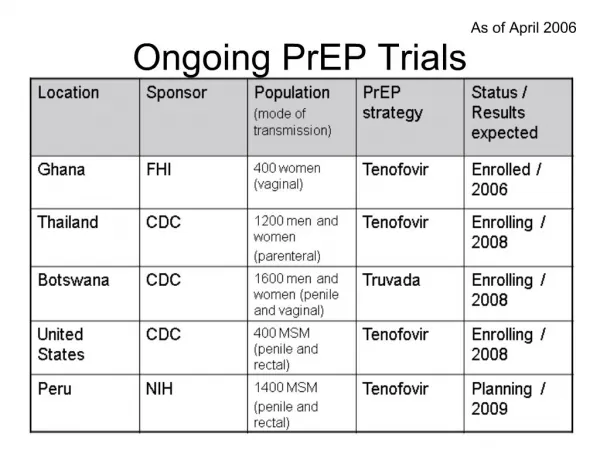
PrEP Trials • Concerns raised about the population effects of daily oral antiretroviral prophylaxis if found to be substantially but not completely effective • Availability and cost • Behavioral disinhibition • Increased prevalence of resistant virus complicating treatment
Phase II/III • 600 men and 600 women • Randomize 1:1 to TDF or placebo daily • Follow monthly for at least 12 months Confirm Safety Determine if TDF works Phase II Phase III Interim Safety Final
How large a problem is TDF resistance likely to be? • Participants could become infected with a virus with TDF resistance mutation(s) by: • Exposure to virus from an HIV-infected person with a mutated virus • Acquisition of wild-type virus and development of resistance mutations while on PrEP with undetected infection
Development of resistance • TDF dispensed monthly • HIV testing done monthly • So max time on TDF monotherapy while infection undetected is 1-2 months
DEVELOP RESISTANCE 1200 on study Resistance in trial participants?An estimate of the numbers
DEVELOP RESISTANCE 1200 on study 600 on TDF Resistance in trial participants?An estimate of the numbers
DEVELOP RESISTANCE 1200 on study 600 on TDF 15 (2.5%) infected Resistance in trial participants?An estimate of the numbers
DEVELOP RESISTANCE 1200 on study 600 on TDF 15 (2.5%) infected If 1% develop resistance < 1 person infected with resistant virus Resistance in trial participants?An estimate of the numbers
INFECTED BY A RESISTANT VIRUS 330,000 HIV+ Resistance in trial participants?An estimate of the numbers
INFECTED BY A RESISTANT VIRUS 330,000 HIV+ 45,000 on HAART Resistance in trial participants?An estimate of the numbers
INFECTED BY A RESISTANT VIRUS 330,000 HIV+ 45,000 on HAART 20,000 in Gabs/FT Resistance in trial participants?An estimate of the numbers
INFECTED BY A RESISTANT VIRUS 330,000 HIV+ 45,000 on HAART 20,000 in Gabs/FT 3060 (15.3%) detectable virus Resistance in trial participants?An estimate of the numbers
INFECTED BY A RESISTANT VIRUS 330,000 HIV+ 45,000 on HAART 20,000 in Gabs/FT 3060 (15.3%) detectable virus 573 (3/16, 19%) with K65R Resistance in trial participants?An estimate of the numbers
INFECTED BY A RESISTANT VIRUS 330,000 HIV+ 45,000 on HAART 20,000 in Gabs/FT 3060 (15.3%) detectable virus 573 (3/16, 19%) with K65R Considering Selection of partners Per act transmission rate ~0 infected with resistant virus Resistance in trial participants?An estimate of the numbers
DEVELOP RESISTANCE 1200 on study 600 on TDF 15 (2.5%) infected If 1% develop resistance < 1 person infected with resistant virus INFECTED BY A RESISTANT VIRUS 330,000 HIV+ 45,000 on HAART 20,000 in Gabs/FT 3060 (15.3%) detectable virus 573 (3/16, 19%) with K65R Considering Selection of partners Per act transmission rate ~0 infected with resistant virus Resistance in trial participants?An estimate of the numbers
Measuring Resistance • All seroconverters continue in follow-up • Genotypic and phenotypic resistance testing will be done for all seroconverters
Trial change • Phase II still underway with TDF alone • Phase III will be done with TDF+FTC daily • Macaque data suggesting better efficacy • PMTCT data suggesting 2 drugs more efficacious than 1 • Few added side effects • Little additional cost • Still one pill per day
Conclusions • Most drug-resistant virus will be generated in the ARV treatment population • The TDF PrEP trials will result in few (if any) additional infections with resistant virus • Treatment alternatives are available in Botswana for trial seroconverters if they acquire resistant virus • The switch to two drugs within the PrEP trial will further lower the risk of infections with resistant virus within trial participants
Contact Dawn K. Smith dks1@cdc.gov +267-390-1696 x210 "The findings and conclusions in this presentation have not been formally disseminated by the Centers for Disease Control and Prevention and should not be construed to represent any agency determination or policy."
Resistant Intermediate Susceptibility Fully Susceptible Study 903: Phenotypic Susceptibility of NRTIs in Presence of K65R (n=8) Fold Change Phenosense Assay (ViroLogic cut-off)