Download
1 / 43
510 likes | 822 Views
Breaking the Vicious Cycle – Safety Considerations for Anemia Therapy. Iain C Macdougall. Anemia Therapies . Red cell transfusions Erythropoiesis-stimulating agents (ESAs) Intravenous iron. Fe complex. The History and Safety of RBC Transfusions.

E N D
Breaking the Vicious Cycle – Safety Considerations for Anemia Therapy Iain C Macdougall
Anemia Therapies Red cell transfusions Erythropoiesis-stimulating agents (ESAs) Intravenous iron Fe complex
The History of RBC Transfusions Began with Hippocrates 400 BC 200 AD Hippocrates Four humors – blood, phlegm, black bile and yellow bile; heart is the central organ Galen Further developed Hippocrates’ ideas and discovered that vessels contain blood
Early Transfusions Used Animal Blood 1600s 1700–1800s William Harvey Blood circulation Richard Lower Blood transfusion in animals Jean-Baptiste Denis Transfused four patients with animal blood, two of whom died First patient-to-patient transfusions are performed
Drawbacks to Blood Transfusions Became Apparent in the 20thCentury 1900–1910 1930–1950s 1970–Present Karl Landsteiner (1901) Documented blood groups A, B and O Oswald Robertson (1917) Established first blood bank using blood group O World War II Blood transfusions used to save thousands of lives Red Cross (1945) Blood collections begin Infection Blood transfusions shown to transmit numerous infections Blood screening becomes vital Supply Despite collections, blood supplies are not inexhaustible
Transfusions Provide an Instant ‘First Aid’ Approach to Treatment of Anemia but at a Risk Risk of infection (parasites, viruses etc)1 Human leukocyte antigen (HLA) sensitization makes kidney transplantation problematic1,2 May be associated with multi-organ failure and increased mortality in critical care patients2,3 Guidelines recommend use of ESAs/i.v. iron to limit transfusions4–6 1. Mak G et al. Curr Treat Options Cardiovasc Med 2008;10:455–464; 2. Weiss G & Goodnough LT. N Engl J Med 2005;352:1011–1023; 3. Vincent JL et al. JAMA 2002;288:1499–1507; 4. Locatelli F et al. Nephrol Dial Transplant 2004;19(suppl 2):ii6–ii15; 5. National Institute for Health and Clinical Excellence. Clinical Guideline 39 (2006); 6.NKF/KDOQITM. Am J Kidney Dis 2006;47(suppl 3):58–70
ESA Research Began over 30 Years Ago 1975–1985 1985–2000 Miyake et al Isolated human erythropoietin (EPO) from large quantities of urine Lin et al Human EPO gene is cloned Recombinant human EPO (RHuEPO) RHuEPO is produced in Chinese hamster ovary cells Eschbach et al; Winearls et al First clinical studies using RHuEPO in hemodialysis population. Success allows physicians to effectively treat renal anemia Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
CREATE CHOIR
CREATE TREAT CHOIR
Besarab A et al. N Engl J Med 1998;339:584–590; Drüeke TB et al. N Engl J Med 2006;355:2071–2084; Singh AK et al. N Engl J Med 2006;355:2085–2098; Pfeffer MA et al. N Engl J Med 2009;361:2019–2032
What have these studies told us? Besarab A et al. N Engl J Med 1998;339:584–590; Drüeke TB et al. N Engl J Med 2006;355:2071–2084; Singh AK et al. N Engl J Med 2006;355:2085–2098; Pfeffer MA et al. N Engl J Med 2009;361:2019–2032
What have these studies told us? ESAs are not the best thing since sliced bread Besarab A et al. N Engl J Med 1998;339:584–590; Drüeke TB et al. N Engl J Med 2006;355:2071–2084; Singh AK et al. N Engl J Med 2006;355:2085–2098; Pfeffer MA et al. N Engl J Med 2009;361:2019–2032
Safety Concerns in the TREAT Study Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT) Randomized, placebo-controlled, double-blind trial: 623 sites, 24 countries, 4038 patients (2012 darbepoetin alfa) Primary endpoint: composite outcomes of death or a cardiovascular event and of death or end-stage renal disease ESA Placebo 0.6 10 8.9§ 8 7.5‡ 7.1 6 Patients (%) 5.0† 4 2.6 2 2.0‡ 1.1 0 Stroke Venous thromboembolic event Arterial thromboembolic event Cancer-related mortality* †, p<0.001 versus placebo ‡, p=0.02 versus placebo §, p=0.04 versus placebo *Amongst patients with a history of malignancy at baseline Pfeffer MA et al. N Engl J Med 2009;361:2019–2032
Safety of ESAs in Oncology Erythropoietin receptors are expressed on many tissues and there is a possibility of cancer progression1–5 Risk of thromboembolism is also of concern in oncology patients treated with ESAs6,7 2.8 2.6 2.4 2.2 Hazard ratio for risk of venous thromboembolism aftertreatment with an ESA6 2.0 1.8 1.6 1.4 1.2 1.0 Metastatic ALL Colon Breast Lung Lymphoma Non-metastatic Error bars = 95% confidence intervals ALL, acute lymphoblastic leukemia 1. Mak G et al. Curr Treat Options Cardiovasc Med 2008;10:455–464; 2. Arcasoy MO et al. Lab Invest 2002;82:911–918; 3. Yasuda Y et al. Carcinogenesis 2003;24:1021–1029; 4. Acs G et al. Am J Pathol 2003;162:1789–1809; 5. Westenfelder C & Baranowski RL. Kidney Int 2000;58:647–657; 6. Hershman DL et al. J Natl Cancer Inst 2009;101:1633–1641; 7. Glaspy P et al. Br J Cancer 2010;102:301–315
New Data Question the Safety of ESAs Nephrology Oncology • Causes Ab+PRCA • Risk of thrombosis • Risk of stroke • Venous thromboembolism • Cancer progression • Risk of thrombosis • Risk of stroke • Venous thromboembolism • Cancer progression 2000–2010 Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130 Ab+PRCA, antibody mediated pure red cell aplasia
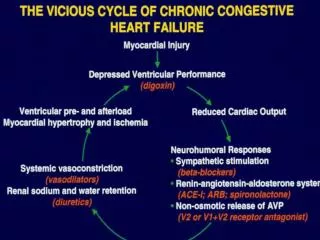
EPO has Non-erythropoietic Actions High EPO levels VSMC [Ca2+]i RAS activation ET-1 Thromboxane Prostacyclin ADMA NO Platelet production Platelet activity E selectin P selectin vWF PAI-1 VSMC proliferation EC proliferation Angiogenesis Blood access stenosis Proliferative retinopathy Vascular remodeling Tumor growth Hypertension Thrombosis VSMC, vascular smooth muscle cell; RAS, renin–angiotensin system; EC, endothelial cell; ADMA, asymmetrical dimethylarginine; PAI-1, plasminogen activator inhibitor; vWF, von Willebrand factor; NO, nitric oxide; ET-1, endothelin-1 Vaziri ND & Zhou X. Nephrol Dial Transplant 2009;24:1082–1088
Hot off the Press… Unger EF et al. N Engl J Med 2010;362:189–192
Benefits of Iron Identified in 17th Century 1600–1900 1900–1940 Sydenham (1681) Value of iron in chlorosis Blaud (1832) Ferrous sulfate pills first manufactured Heath (1932) First i.v. injection of iron salts to treat anemia Auerbach M et al. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
I.v. Iron Salts / Colloids → Carbohydrates 1940s Goetsch (1946) I.v. colloidal Fe(OH)3 for anemia. Severe toxic reactions in patients: ‘preclude use for therapeutics’ Nissim (1947) Use of i.v. iron saccharide Auerbach M et al. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
I.v. Iron Salts / Colloids → Carbohydrates Iron oxyhydroxide core Carbohydrate shell 1940s Goetsch (1946) I.v. colloidal Fe(OH)3 for anemia. Severe toxic reactions in patients: ‘preclude use for therapeutics’ Nissim (1947) Use of i.v. iron saccharide Auerbach M et al. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
I.v. Iron Salts / Colloids → Carbohydrates 1950s 1980s 1940s Goetsch (1946) I.v. colloidal Fe(OH)3 for anemia. Severe toxic reactions in patients: ‘preclude use for therapeutics’ Nissim (1947) Use of i.v. iron saccharide I.v. iron sucrose Launched in Switzerland Baird & Podmore (1954) I.m. iron dextran (Imferon) → I.v. Auerbach M et al. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
I.v. Iron Salts / Colloids → Carbohydrates 1950s 1980s Anaphylaxis DEATH 1940s Goetsch (1946) I.v. colloidal Fe(OH)3 for anemia. Severe toxic reactions in patients: ‘preclude use for therapeutics’ Nissim (1947) Use of i.v. iron saccharide I.v. iron sucrose Launched in Switzerland Baird & Podmore (1954) I.m. iron dextran (Imferon) → I.v. Auerbach M et al. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
I.v. Iron Salts / Colloids → Carbohydrates 1950s 1980s 1940s Goetsch (1946) I.v. colloidal Fe(OH)3 for anemia. Severe toxic reactions in patients: ‘preclude use for therapeutics’ Nissim (1947) Use of i.v. iron saccharide I.v. iron sucrose Launched in Switzerland Baird & Podmore (1954) I.m. iron dextran (Imferon) → I.v. Hamstra (1980) Anaphylactoid adverse events (AEs) to iron dextran are ‘serious and unpredictable’. Leads to black box label and test dose Shuttleworth (1983) Meningism legal case leads to the recall of the world’s supply of Imferon Auerbach M et al. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130
Oral Versus I.v. Iron 1990s–2010 Oral iron safety concerns Highly unlikely that patients will experience a life-threatening AE, however, compliance is very low due to gastrointestinal side effects AEs affecting compliance are more common in patients taking oral iron as opposed to i.v. iron1,2 Other i.v. iron Licensing of non-dextran i.v. iron preparations in US (sucrose, gluconate) Next generation Ferric carboxymaltose and ferumoxytol have recently been developed Adapted from Auerbach M. Am J Hematol 2008;83:580–588; Macdougall IC & Ashenden M. Adv Chronic Kidney Dis 2009;16:117–130; 1. Spinowitz BS et al. J Am Soc Nephrol 2008;19:1599–1605; 2. Qunibi W et al. XLV ERA-EDTA Congress, 10–13 May 2008, Stockholm, Sweden. Abstract MO018
New I.v. Iron Preparations are Associated with Fewer AEs Compared with Oral Iron Spinowitz et al 20081 Open-label, randomized, controlled, multicenter, Phase III trial 292 patients in the safety population 217 ferumoxytol 75 ferrous fumarate Qunibi et al 20082 Randomized, controlled, multicenter trial 250 patients 147 ferric carboxymaltose 103 ferrous sulfate I.v. iron Oral iron 30 26.2 25 24.0 20 Patients experiencing drug-related AEs (%) 15 10 10.6 5 2.7 0 Spinowitz et al 2008 Qunibi et al 2008 1. Spinowitz BS et al. J Am Soc Nephrol 2008;19:1599–1605; 2. Qunibi W et al. XLV ERA-EDTA Congress, 10–13 May 2008, Stockholm, Sweden. Abstract MO018
There are Potential Concerns About the Use of I.v. Iron Short-term Anaphylactic reactions (iron dextran only; dextran Abs) ‘Free iron’ reactions (all i.v. irons – too much, too quickly)
Iron Dextran has the Highest Reporting Rates in all Clinical Categories 2.5 Urticaria 2 Upper airway angioedema Anaphylactoid reaction 1.5 Reports/million 100 mg iron dose equivalents Anaphylaxis 1 0.5 0 Iron dextran Iron sucrose Sodium ferric gluconate Bailie GR et al. Nephrol Dial Transplant 2005;20:1443–1449
I.v. Iron Preparations Differ in AE Profiles Total 400 Life-threatening 331 300 269 232 Number of major AEs reported (2001–2003) 175 200 100 29 22 11 5 0 Sodium ferricgluconate High MWiron dextran Low MWiron dextran Iron sucrose Total number of doses dispensed: 11.97 million 2.56 million 6.69 million 8.84 million Chertow GM et al. Nephrol Dial Transplant 2006;21:378–382
There are Potential Concerns About the Use of I.v. Iron Short-term Anaphylactic reactions (iron dextran only; dextran Abs) ‘Free iron’ reactions (all i.v. irons – too much, too quickly) Long-term Increased susceptibility to infection Increased oxidative stress Iron overload
Iron Administration is not Associated with Increased Infection Risk Iron overload bacterial growth / virulence PMN phagocytosis / bacterial killing Animals Parenteral iron administered to rats or mice with active infection harmful
Iron Administration is not Related to Infection Hoen et al 2002: Data from prospective study of 985 HD patients Risk factors for bacteremia analyzed I.v. iron administration does not significantly increase the risk of bacteremia in chronic HD patients Hoen B et al. Clin Nephrol 2002;57:457–461
Iron is a Redox Metal which might Cause Oxidative Stress Fe3+ (Ferritin) Fe2+ Fenton reaction OH- radical ROS Macromolecules(membrane lipids) Lipid-derived free radicals Atherosclerosis ROS, reactive oxygen species
I.v. iron 200 * Control ** 150 ** 100 Total peroxides (µmol/L) 50 0 C D A B A, before HDB, after HD or immediately after i.v. iron C, 1 hr after the collection of sample B D, before the next HD session *p<0.01; **p<0.001 Scheiber-Mojdehkar B et al. J Am Soc Nephrol 2004;15:1648–1655
Cohort study • – 32,566 HD patients (Fresenius dialysis centers) • – All-cause mortality • – 2-year follow-up • – Multivariate models to account for timing of i.v. iron and also co-morbidity Feldman HI et al. J Am Soc Nephrol 2004;15:1623–1632
Iron Dose, Unlike Low Albumin, is not Linked to Increased Mortality in HD Probability of mortality (Adjusted hazard ratio ± 95% CI) 0 1 2 3 4 5 0–700 Cumulative 6 month iron dose (mg) 700–1000 1000–1800 >1800 <3.0 3.0–<3.5 Albumin(g/dL) 3.5–<4.0 4.0–<4.5 Results for both covariates are from unlagged time-dependent model Adapted from:Feldman HI et al. J Am Soc Nephrol 2004;15:1623–1632
Conclusions • RBC transfusions risks infection and HLA sensitization1,2 • ESAs are associated with increased risk of thromboembolic events, stroke and cancer progression3–5 • Oral iron is associated with significantly greater rates of AEs compared with i.v. iron6,7 • Life-threatening AEs in response to i.v. iron administration are rare8,9 • Regarding safety, not all i.v. iron preparations are the same8,9 Are the newer i.v. preparations ‘safer’ than the older i.v. iron compounds? 1. Weiss G & Goodnough LT. N Engl J Med 2005;352:1011–1023; 2. Mak G et al. Curr Treat Options Cardiovasc Med 2008;10:455–464; 3. Pfeffer MA et al. N Engl J Med 2009;361:2019–2032; 4. Singh AK et al. N Engl J Med 2006;355:2085–2098; 5. Szczech LA et al. Kidney Int 2008;74:791–798; 6. Spinowitz BS et al. J Am Soc Nephrol 2008;19:1599–1605; 7. Qunibi W et al. XLV ERA-EDTA Congress, 10–13 May 2008, Stockholm, Sweden. Abstract MO018; 8. Bailie GR et al. Nephrol Dial Transplant 2005;20:1443–1449; 9. Chertow GM et al. Nephrol Dial Transplant 2006;21:378–382